“Calkins told delegates that there are 120 trials involving AF ablation listed on Clinicaltrials.gov. Of these, 83 are catheter ablation trials – 72 involving available ablation technology and 11 involving new technologies. “Twelve are completed, 36 are enrolling, 14 are inactive, four terminated or suspended, and six are pending,” he said. “It is interesting that 49 are hospital-funded trials, 25 funded by industry, and three by the National Heart, Lung and Blood Institute.”
_____________________
http://www.massdevice.com/news/st-jude-lands-approval-gps-enhancements-its-ablation-catheters
_____________________
This inconsistency of catheter ablation in achieving basic technical goals impacts on the results of the procedure. A recent study employing rigorous follow-up show that catheter ablation succeeded in long-term restoration of sinus rhythm without anti-arrhythmia drugs in only 34% of patients.3 A second study of only paroxysmal AF patients, who are relatively easy to cure, resulted in long-term success in only 57%, with a serious complication rate of 12%.4 This compares to the 95% published effectiveness of the five-box thoracoscopic maze in curing longstanding persistent atrial fibrillation, the most difficult group of patients to treat.5
http://www.ohioafib.com/catheter-ablation.cfm
________________________
____________
But, Dr. Wing added, “You do a study because you don’t know the answer.” http://www.nytimes.com/2012/10/20/health/in-study-weight-loss-did-not-prevent-heart-attacks-in-diabetics.html?ref=todayspaper
_________________
Calkins Success rate 29% No Cure….
“Sobering” long-term outcomes following ablation of atrial fibrillation
JANUARY 5, 2011
Bordeaux-Pessac, France – New data from one of the groups that pioneered the catheter-ablation approach for the treatment of atrial fibrillation provides a revealing look at the long-term results of the radiofrequency procedure. Arrhythmia-free survival rates after a single catheter-ablation procedure are relatively low at five years, just 29%, but the long-term success increases to 63% when outcomes are measured after the last ablation procedure.
http://www.theheart.org/article/1168671.do
_____________
On Wednesday, October 21, 2009 the Medicare Evidence Development & Coverage Advisory Committee (MedCAC) is holding Catheter Ablation for the Treatment of Atrial Fibrillation, a meeting to discuss the adequacy of the available evidence for the use of catheter ablative techniques to treat patients with atrial fibrillation. Hugh Calkins whoring for industry:http://www.hrsonline.org/Policy/ICDRegistry/upload/MedCAC-Comments-09-21-09.pdf
______________
Agonizing Choices for Heart Patients (Medtronic Leads)
The other jaw-dropper was the 2007 COURAGE trial examining patients with stable coronary artery disease, or hardening of the arteries. It found that a widely performed procedure called percutaneous coronary intervention, usually involving the insertion of tiny metal scaffolds called stents to prop arteries open, did not reduce incidence of death or heart attacks in these patients.
Those two treatments “cost billions of dollars and supported the existence of entire specialties for many years,” Ioannidis and his co-authors wrote in January in the Journal of the American Medical Association. Ioannidis says the data clearly show that patients were subjected to risk with no chance of benefit. While the number of prescriptions for combination hormone therapy dropped 80 percent or more in the years after the WHI study, the number of coronary interventions did not decline nearly as dramatically following the COURAGE trial. “Defenders of these therapies and interventions wrote rebuttals and editorials and fought for their specialties, but the reality was that the best that could be done was to abandon ship,” Ioannidis wrote in JAMA.
Before Palmaz could finish his work, though, the government funding that backed his research dried up. Yet Palmaz was blessed with fortuitous timing. Around the same time he was developing his prototype, Congress passed a law that attempted to acknowledge how ineffective the government had been at developing medical research into real, commercially available treatments. The law gave doctors and companies incentives to bring new technology to market by allowing them to profit from the investment of their time and money.
Fraud by major drug companies is rampant: http://bottomline.msnbc.msn.com/_news/2012/03/06/10591103-drug-makers-have-paid-out-billions-for-fraud-report-shows WHO Leader on compelling need to manage antibiotic use: http://www.independent.co.uk/life-style/health-and-families/health-news/health-chief-warns-age-of-safe-medicine-is-ending-7574579.html
some things should be kept in mind when praising Pronovost: Pronovost’s 5-step checklist was neither unique nor innovative. It basically was/is nursing 101. Also, his checklist only involved insertion of CLCs and included no maintenance bundle. The literature is clear that some 70% of CLIs occur during what is called the “maintenance phase.” Also, Pronovost’s Keystone Initiative was limited and failed to call for universal implementation. His group received $millions, in addition to the accolades, such as among “the top 100 most powerful….” Having said all of this, I suppose someone promoting half measures is better than having nothing at all. But I remain unimpressed by an industry that can only find this to heap praises upon while thousands continue to suffer and die from the utter failure of leadership. Pronovost may think patient safety a “dream,” patients think of it as life and death. And they are terrified. *** To add to what you said, and I am repeating myself here…..it is now rare to test a central line tip (the part removed from the body)….this use to be the standard for ruling in a central line infection. I have asked at repeated hospital ICU’s, “Should we culture the central line tip?” When my critical patient begins to show signs and symptoms of infection/sepsis (not admitting diagnosis), I have to call/notify the physician of the symptoms/labs/positive blood cultures, etc. I really do not want to have to call again, so if I am not given appropriate/complete orders, I ask for them. I am told, “No, it is too late, the infection is already there, it will not mean the central line tip is the origin.” In fact, I have only been told to send one central line tip for a culture in the last three years. The ‘list’ has really helped the insertion process, most physicians are following it, maybe 75% that I see (and I assist with a ton of insertions). However, the criteria for ruling in a central line infection has changed so when we compare results we are comparing apples and oranges. Maybe someone could find out for us how many central line tips were cultured ( on an average) before the infamous ‘list’ came out, and how many are cultured now. I think it would be shocking _______________ ______________ But if doctors give treatment with the intent to gain knowledge, they are technically doing research, which must receive IRB approval. _______
_______
http://www.wiltsglosstandard.co.uk/news/9541429.Gloucestershire_man_died_after_heart_operation__inquest_hears/ _______ In Maryland, Johns Hopkins Bayview Medical Center in Baltimore, Maryland paid $2.8 million to settle qui tam allegations that it reported false secondary diagnoses for its inpatient hospital stays to Maryland’s hospital rate setting commission, resulting in inflated reimbursement rates to the hospital. These false diagnoses included claims that patients suffered from malnutrition and acute respiratory failure when those conditions had not actually been diagnosed or treated during the patients’ hospital stay.http://www.justice.gov/archive/dag/pubdoc/hcfacreport2009.pdf _____ Endoscopic Technologies Inc. (Estech), a medical device manufacturer, paid $1.4 million to resolve civil qui tam allegations that it marketed its surgical ablation devices to treat atrial fibrillation (the most common cardiac arrhythmia or abnormal heart rhythm), a use that is not approved by the FDA. The government also alleged that Estech promoted expensive heart surgeries using the company’s devices when less invasive alternatives were appropriate, advised hospitals to up-code surgical procedures using the company’s devices to inflate Medicare reimbursements, and paid kickbacks to healthcare providers to use its devices. http://www.justice.gov/archive/dag/pubdoc/hcfacreport2009.pdf ____________ Radiation Exposure: A Silent Complication of Catheter Ablation Procedures
- Mahmoud Houmsse,aMD, FHRS
,
- Emile G. Daoud, MD, FHRS

Received 22 January 2012 published online 30 January 2012. http://www.heartrhythmjournal.com/article/S1547-5271(12)00074-4/pdf
_____________ ATRICURE APPEAL TEMPLATE (To be printed on the physician’s letterhead. Please insert specific evidence of medical necessity from the patient’s medical record) April 9, 2007 Coventry Healthcare of Delaware, Inc. Attention: Appeals Coordinator 2751 Centerville Road Suite 400 Wilmington, Delaware 19808 RE: Pre-Service Appeal CPT 33255 is medically necessary. Please call me at your earliest convenience to understand the numerous patient benefits. Patient: Subscriber ID#: Date of Birth: Facility: Address: Dear Appeals Coordinator: The purpose of this letter is to establish the medical necessity of a procedure that I must perform on your subscriber as soon as possible. Last week, Coventry issued a pre-service denial and I would like a board-certified cardiothoracic surgeon to review this request for reconsideration. CPT 33255 [Operative tissue ablation and reconstruction of atria, extensive (e.g. maze procedure); without cardiopulmonary bypass]is medically necessary. In view of numerous CPT coding changes that took effect on January 1, 2007, I am hopeful this pre-service denial was simply the result of a miscommunication? As you may know, the AMA released five new CPT codes in the Surgery/Cardiovascular “Electrophysiologic Operative Procedure” section of CPT 2007. I am not performing an investigational/experimental procedure. The CPT code I selected is not a Category III T-code used for tracking new and emerging technologies. I selected a fully-valued Level I CPT code recently surveyed by the Society of Thoracic Surgeons (STS) in 2006 and released by the AMA in 2007. Please consult with a cardiothoracic surgeon, the STS and/or AMA to better appreciate that tissue ablation can be accomplished by many different methods. Simplification of the maze procedure has been made possible by different ablation techniques. The acceptance of alternative energy technology that shortens and simplifies the surgical management of atrial fibrillation (AF) was the reason behind these new CPT codes. The “cut-and sew” maze CPT code 33253 was deleted in 2006 and replaced with 5 new CPT codes to better match contemporary surgical practice. While some payers continue to view the classic “cut-and-sew” Cox-maze procedure to be the surgical “gold standard”, it is very important that you fully appreciate the risks associated with this lengthy, complex and difficult procedure. The requirement for cardiopulmonary bypass (CPB) and the technical difficulty of this approach have limited its use Everyday in clinical practice, cardiothoracic surgeons create alternative lines of conduction blocks with improved technology without the known morbidity associated with a full sternotomy and CPB. If Anthem BCBS, the largest private payer in the U.S, considers this CPT code and ICD-9-CM Procedure Code 37.33 (excision or destruction of other lesions or tissue of heart open approach/ trans-thoracic approach) to be medically necessary for drug resistant atrial fibrillation or flutter, then so should you. Anthem’s medical policy for the Maze procedure is attached for your review and consideration. My surgical plan for your subscriber is to use an ablative device that delivers targeted bi-polar radiofrequency energy to create discrete linear transmural lesions. Contrary to your maze medical policy, I am NOT performing a catheter ablation! Your medical policy is not in step with contemporary cardiovascular surgical practice for the treatment of persistent AF. It is outdated and in need of immediate revision. For example, it currently identifies the deleted maze CPT code 33253 as a covered benefit. Besides reviewing CPT 2007, please consult with a board certified cardiothoracic surgeon and/or me for a peer-to-peer discussion of the references cited on the enclosed bibliography. Your subscriber needs surgery now! Early intervention will increase the likelihood of restoring this patient to normal sinus rhythm. The most significant predictor of long-term AF recurrence is the duration of pre-operative AF. While the classic cut-and-sew maze procedure is extremely effective, it has been supplanted by newer operations that rely on alternate energy, such as radiofrequency, to create lines of conduction block In a systematic review of the surgical treatment of AF, Khargi et al (2005) could not identify any significant difference in the post-op sinus rhythm conversion rates between classic “cut & sew” Cox-Maze technique that requires an open sternotomy versus alternative energy sources, such as radiofrequency, which simply requires trans-thoracic incisions. The surgical objective through an open sternotomy with CPB or trans-thoracic incisions is the same – to interrupt the aberrant atrial conduction pathways in the heart that are causing the patient’s atrial fibrillation. The expected outcomes from either approach is to restore normal sinus rhythm and prevent ischemic stroke. Availability of alternative energy sources to create lesions sets has virtually eliminated the need for the cut-and-sew Cox-maze procedure. The clinical and economic gains associated with avoiding a full sternotomy and CPB are quite significant to me, my patient, and your health plan. CLINICAL JUSTIFICATION Atrial fibrillation (AF) is the most commonly occurring cardiac arrhythmia. It affects more than 2.5 million people in the United States, and its prevalence rises with age. It is associated with numerous cardiac morbidities, decreased quality of life and decreased survival. Symptoms include palpitations, decreased exercise tolerance and dyspnea. Stroke is the most feared complication of atrial fibrillation. It is well-known that patients with AF are five times more likely to suffer a stroke than patients in normal sinus rhythm. Among patients with AF, there is a 5% annual risk of stroke. Per 2006 ACC/AHA/ESC Practice Guidelines for the “Management of Patients with Atrial Fibrillation”, the inconsistent efficacy and potential toxicity of antiarrhythmic drug therapies have established the need for non-pharmacologic treatments in patients with persistent AF who fail to respond to anti-arrhythmic drug therapy. Your subscriber is an ideal candidate for an operative tissue ablation through a trans-thoracic approach (ICD-9-CM Procedure code 37.33), but as shown below, time is of the essence for this patient’s well-being. SUBSCRIBER’S MEDICAL NECESSITY (Please insert specific information about the patient, such as age, chief compliant, current medications, significant events in the past medical history, employment status, family issues). For example, this is a 46 year old independent contractor, who has suffered with AF for more than 5 years despite taking numerous anti-arrhythmics. While this patient recognizes the need for surgery, he can not afford to be out-of-work for 8-12 weeks following an open surgical procedure. With a trans-thoracic approach, I anticipate he can return to work for within 2-3 weeks. Upon your review of the enclosed NEW evidence, please do not hesitate to call me with any further questions to better appreciate the medical necessity of this surgery. I would be very happy to share additional clinical information, as well as provide further evidence regarding the effectiveness of operative tissue ablation and reconstruction of the atria through a trans-thoracic incision. In advance, thank-you for your time and re-consideration. At your earliest convenience, I await your reply in writing. Sincerely, Name of Surgeon Phone: Citations in the peer-reviewed literature that establish the medical necessity of CPT 33255 Barnett SD, and Ad N. Surgical ablation as treatment for elimination of atrial fibrillation: a META analysis. J Thorac Cardiovasc Surg2006;131:1029-35. Benjamin EJ, et al. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998 Sep 8;98(10):946-52. Cox JL. The surgical treatment of atrial fibrillation. IV. Surgical technique. J Thorac Cardiovasc Surg 1991 ;101 :584-92. Doukas G, et al. Left atrial radiofrequency ablation during mitral valve surgery for continuous atrial fibrillation: a randomized controlled trial. JAMA 2005 Nov 9;294(18):2323-9. Fuster V, et al. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation. JACC 2006;48(4):e149-246. Gaynor SL, et al. Surgical treatment of atrial fibrillation: predictors of late recurrence. J Thorac Cardiovasc Surg 2005 Jan;129(1):104-11). Gaynor SL, et al. A prospective, single-center clinical trial of a modified Cox maze procedure with bipolar radiofrequency ablation. J Thorac Cardiovasc Surg 2004 Oct; 128(4):535-42. Gillinov AM and Saltman AE. Ablation of atrial fibrillation with concomitant cardiac surgery. Semin Thorac Cardiovasc Surg. 2007 Spring; 19 (1): 25-32. Gillinov AM. Advances in surgical treatment of atrial fibrillation. Stroke.2007 Feb; 38 (2 Suppl): 618-23. Gillinov AM et al. Surgery for permanent atrial fibrillation: impact of patient factors and lesion sets. Ann Thorac Surg. 2006 Aug; 82 (2): 502-13. Gillinov AM, Wolf RK. Surgical ablation of atrial fibrillation. Prog Cardiovasc Dis. 2005 Nov-Dec;48(3):169-77. Gillinov AM. Ablation of atrial fibrillation with mitral valve surgery. Curr Opin Cardiol. 2005 Mar;20(2):107-14. Gillinov AM, et al. Stapled excision of the left atrial appendage. J Thorac Cardiovasc Surg 2005 Mar;129(3):679-80. Gillinov AM, et al. Surgical ablation of atrial fibrillation with bipolar radiofrequency as the primary modality. J Thorac Cardiovasc Surg. 2005 Jun;129(6):1322-9. Gillinov AM, McCarthy PM. Advances in the surgical treatment of atrial fibrillation. Cardiol Clin. 2004 Feb;22(1):147-57. Gillinov AM, McCarthy PM. Curative surgery for atrial fibrillation: current status and minimally invasive approaches. Expert Rev Cardiovasc Ther.2003 Nov;1(4):595-603. Gillinov AM, et al. Contemporary treatment for atrial fibrillation. Pacing Clin Electrophysiol. 2003 Jul;26(7 pt 2):1641-4. Gillinov AM, McCarthy PM. Atricure bipolar radiofrequency clamp for intraoperative ablation of atrial fibrillation. Ann Thorac Surg 2002 Dec;74(6):2165-8. Gillinov AM, Blackstone EH, McCarthy PM. Atrial fibrillation: current surgical options and their assessment. Ann Thorac Surg. 2002 Dec;74(6):2210-7. Hart RG, Halperin JL, et al. Lessons from the stroke prevention in atrial fibrillation trials. Ann Intern Med. 2003 May 20; 138(10):831-8. Khargi K et al. Surgical treatment of atrial fibrillation: A systemic review.Eur J Cardiovasc Surg. 2005; 129 (1) 104-111. Lemery R, Guiraudon G. Catheter and surgical ablation strategies in atrial fibrillation: what have we learned? Curr Opin Cardiol.2005;20(1)26-30. Misaki T et al. Recent topics on the surgical treatment for atrial fibrillation. Ann Thorac Cardiovascular Surg. 2004; 10 (5):277-280. Mokadam NA, et al. A prospective multicenter trial of bipolar radiofrequency ablation for atrial fibrillation: early results. Ann Thorac Surg 2004 Nov;78(5):1665-70. Pruitt JC, et al. Totally endoscopic ablation of lone atrial fibrillation: initial clinical experience. Ann Thorac Surg 2006 Apr;81(4):1325-30.
_____________________ Patient-Centered Outcomes Research Institute (PCORI) Governing Board Conflicts of Interest Information http://www.gao.gov/about/hcac/patientcentered_conflicts.html _________________ Cardima Revelation pass through payments ____________________ http://lifeyousave.com/excerpt.html _______________ Distribution: http://www.newswise.com/contact?topic=distribution&subject=Becoming%20a%20Contributor ___________________ GOOD SITE: http://www.newswise.com/channels/rss _________________ Good luck with the procedure. I had 2 ablations in the past 4 months,and both of my arrhythmias have now returned. http://blogs.webmd.com/heart-disease/2012/01/john-edwards-has-a-heart-condition.html ____________ Ablation fix short-lived: http://www.reuters.com/article/2012/01/06/us-heart-rhythm-idUSTRE80520O20120106 ___________________ Grove article for Helen (Open heart surgery to retrieve Lasso) _______________________ Johns Hopkins Malpractice: On February 5, 2010, a Baltimore City jury returned a verdict in the amount of $250,000.00 against Johns Hopkins Hospital and in favor of the parents of a 17-year-old girl who suffered from a rare disorder which prevents her body from aging. Brooke Greenberg a retired Chicago real estate attorney had been a long-standing patient at Hopkins, which treated her regularly for her condition. She was scheduled for surgery to replace her feeding tube in March of 2007. Her father discovered her unattended in a swing in a hallway with inexplicable bruising. The jury was likely swayed by the conflicting testimony of the nurses called to testify, the alterations to the medical records and the photographic evidence of the injuries. http://www.marylandmalpracticelawyers.com/2010/02/25000000-malpractice-verdict-against-johns-hopkins-hospital.html _______________ http://www.medscape.com/viewarticle/757097?src=rss Jan 2012 “I’m not telling you this to discourage you from developing a program–I’m telling you this to say if you’re going to do it, you need to think about it as a full-time job as opposed to a part-time thing to dabble at,” Horton explained. “Developing an afib program is really a long-term process. It takes almost a year of preparation time to even start it and then another four years of database acquisition to have [enough data] to even talk about.” Developing a prospective database _______________ Jan 2012 New AF Guidelines HRS: New AF Ablation Consensus Doc Previewed Heartwire http://mp.medscape.com/cgi-bin1/DM/t/hDcos0OsnUz0c8L0I32U0Ej _____________ Biosense Webster Announces FDA approval of the THERMOCOOL(R) SF Catheter in the United States http://www.marketwatch.com/story/biosense-webster-announces-fda-approval-of-the-thermocoolr-sf-catheter-in-the-united-states-2012-01-11 _________________ In Maryland, Johns Hopkins Bayview Medical Center in Baltimore, Maryland paid $2.8 million to settle qui tam allegations that it reported false secondary diagnoses for its inpatient hospital stays to Maryland’s hospital rate setting commission, resulting in inflated reimbursement rates to the hospital. These false diagnoses included claims that patients suffered from malnutrition and acute respiratory failure when those conditions had not actually been diagnosed or treated during the patients’ hospital stay. http://www.justice.gov/archive/dag/pubdoc/hcfacreport2009.pdf
Mortality rate a misleading quality measure Mortality rate a misleading quality measure
Despite being widely used as measure for quality, mortality rates may be a misleading quality indicator because hospitals use varied accounting methods, according to a new study published inClick here to read more on our site Yes, it is remarkable if this has not been taken into account in the reporting. Short hospital stay – i.e., high patient volume – is the reason no advances have been made in patient safety. I recently chanced to find the number of discharges from MUSC where my son died. The hospital has the same number of beds – 530 – as it did ten years ago. But the number of discharges (29,000+) is more than double the number in 2000 (13,000+). They couldn’t handle 13,000. I can’t imagine what they are doing with 29,000.
____________________________
Ablation for Afib Dogged by Complications
http://www.medpagetoday.com/Cardiology/Arrhythmias/30461
_______
(12) OHRP expressed concern that there appears to be boilerplate informed consentformatting that may be confusing to subjects. http://www.scribd.com/doc/54401548/ohrp-uw-0905
_________
Complications of Atrial Fibrillation Ablation When Prevention Is Better Than Cure
____ __ Who Was to Blame for the Botched Malpractice Settlement? Good story http://www.outpatientsurgery.net/news/2011/12/11-Who-Was-to-Blame-for-the-Botched-Malpractice-Settlement ________________ http://retractionwatch.wordpress.com ________________ About one year ago, the first AF ablation catheter, the Navistar Thermocool, was granted FDA approval (Medical Device Daily, Feb. 9, 2009). Developed by the Biosense Webster (Diamond Bar, California) division of Johnson & Johnson (J&J; New Brunswick, New Jersey), it was cleared for the treatment of drug refractory recurrent symptomatic paroxysmal (PAF, intermittent early stage) atrial fibrillation. Catheter ablation, which before that approval was practiced on an “off-label” basis, was now legitimized by that approval and it remains the mainstay of device-based treatment of AF. http://www.haimovitchmedtech.com/articles-cardiology-2010-boston-symposium.html __________________ Patient story: I let my cardiologist talk me into a flutter ablation even though I was scheduled for an ablation with Dr Natale in SF on the beginning of October. I arrived at the medical center on June 28, 2011. The flutter ablation went so well he decided to do the atrial fibrillation. He knew I was scheduled for that procedure with Dr Natale. It is assumed one of the catheters hungup on the mitral valve and it was pulled loose. They tried reparing the valve without success. my blood pressure and heart rate became so slow the doctor told my family he did not thing I would make it. The blood pressure raised enough the next day that they replaced the valve. then everything else started to happen. My kidneys shut, then my lungs. I was hooked up to every machine they had. Again, the Doctors did not think I would make it. i spent ten days in ICU and another five weeks in the hosbital. It was a nightmare for my family. I am 64 years old and recovery has been slow. I was in a semi-coma for five weeks. I had to learn to walk again. I am finally starting to get back to normal. I am on Cumadin, flecinade, and diltizem. The fast heart rate is gone, but atrial fibrillation comes and goes. I use a walker to get around the house. Please choose your doctor well! http://www.afibbers.net/forum/read.php?f=9&i=12256&t=12256 ________________ Calkins Medtronic Stock Fraud: http://securities.stanford.edu/1038/MDT_01/2008418_r01o_0704564.pdf 77. The letter also failed to disclose that the so-called “Independent Physician Quality Panel” (the “Independent Panel”) that supposedly had reviewed the Fidelis fracture reports and assisted the Company with its investigation, was not in fact “independent” because half of its members had conflicts of interest which compromised their objectivity and made them beholden to Medtronic. In particular, the Independent Panel consisted of doctors R. Hardwin Mead, Steven J. Compton, Kevin Hackett, Hugh Calkins, John DiMarco and Mariell Jessup. ________________ Calkins on death by ablation: Results: Thirty-two deaths (0.98 per 1,000 patients) were reported during 45,115 procedures in 32,569 patients. Causes of deaths included tamponade in 8 patients (1 later than 30 days), stroke in 5 patients (2 later than 30 days), atrioesophageal fistula in 5 patients, and massive pneumonia in 2 patients. Myocardialinfarction, intractable torsades de pointes, septicemia, sudden respiratory arrest, extrapericardial pulmonary vein (PV) perforation, occlusion of both lateral PVs, hemothorax, and anaphylaxis werereported to be responsible for 1 death each, while asphyxia from tracheal compression secondary to subclavian hematoma, intracranial bleeding, acute respiratory distress syndrome, and esophageal perforation from an intraoperative transesophageal echocardiographic probe were causes of 1 late death each…. devastating complications may occasionally occur, some of them ultimately leading to death of the patient (5,7). Systematic assessment of death rates and precipitating causes is difficult, because of the rare occurrence of death, making its description anecdotal in single-center reports (8–10), and because of reluctance to publicize this information (7). As a consequence, physicians performing CA of AF sometimes discuss this complication, but a clear picture about its incidence in the real-world practice is lacking. http://content.onlinejacc.org/cgi/content/full/53/19/1798During the presentation, Calkins said the two current treatment options for AF, including conventional radiofrequency ablation catheters, are not designed well enough to treat persistent AF, given that persistent patients often have multiple triggers, rotors, and drivers of the arrhythmia within the atrium. These catheters are time-consuming to use, as physicians create lesions in different areas, but the Medtronic catheter system is a multielectrode device, so they are able to ablate multiple areas of the left atrium much more easily. Wrapping up the panel meeting, Yancy said that despite the negative vote on risks and benefits, it simply can’t be approved “yet.” Better safety results, as well as possible technical tweaks to the catheter, are needed, he said.
___________________________________________
Complications of Atrial Fibrillation Ablation When Prevention Is Better Than Cure
Article | 2006-12-17
Devices Can Interfere With Peaceful Death :Implants Repeatedly Shock Hearts Of Patients Who…
Rob Stein, A01 (Post)
- …When Carol Lewis’s father-in-law died, family members circled his hospital bed to pray, expecting to offer their final goodbyes…
RESS RELEASE
Nov. 14, 2011, 8:00 a.m. EST
Negative FDA Panel Decision on Medtronic Unlikely to Lessen Demand for an Improved Treatment Method for Atrial Fibrillation Market for Atrial Fibrillation Treatments Will Remain Strong, According to Millennium Research Group http://www.marketwatch.com/story/negative-fda-panel-decision-on-medtronic-unlikely-to-lessen-demand-for-an-improved-treatment-method-for-atrial-fibrillation-2011-11-14http://www.marketwatch.com/story/negative-fda-panel-decision-on-medtronic-unlikely-to-lessen-demand-for-an-improved-treatment-method-for-atrial-fibrillation-2011-11-14 _______ FDA Public hearing transcript Sept. 20111: http://www.fda.gov/downloads/MedicalDevices/NewsEvents/WorkshopsConferences/UCM275006.pdf THE WALL STREET JOURNAL FDA Scientists Ask Obama to Restructure Drug Agency http://online.wsj.com/article/SB123142562104564381.html By Alicia Mundy And Jared A. Favole WASHINGTON — A group of scientists at the U.S. Food and Drug Administration on Wednesday sent a letter to President-elect Barack Obama’s transition team pleading with him to restructure the agency, saying managers have ordered, intimidated and coerced scientists to manipulate data in violation of the law. _____________ Medicare payment for Cardima Revelation Program Memorandum Department of Health and Human Services (DHHS) Intermediaries HEALTH CARE FINANCING ADMINISTRATION (HCFA) Transmittal A-01-17 Date: JANUARY 31, 2001 C2104 Catheter, electrophysiology, Lasso Deflectable Circular Tip Mapping Catheter, Cardima Tracer Over-the-Wire Mapping Microcatheter, Cardima PathFinder Microcatheter, Cardima Revelation Microcatheter The Status of Donor Nephrectomy (2005) Donna L. Luebke, CNP MetroHealth Medical Center Cleveland, OH The first living kidney donor surgery was performed over 50 years ago. Until 1995, this procedure required an 8-12 inch flank incision. Although open nephrectomy has a reported low morality (0.03%), it has a substantial morbidity with complication rates ranging from 15-20% or higher (Barlett, 1999) which includes flank hernia (near 9%), pneumothorax 8%, chronic wound bulging or diastasis (occurring in as many as 25% of patients.) Return to normal activity could be up to 8 weeks. The limitations of open nephrectomy combined with the success of other laparoscopic procedures provided the impetus for live donor laparoscopic nephrectomy, a minimally invasive surgery. In 1995, Ratner and Kauvossi performed the first successful laparoscopic live donor nephrectomy atJohnsHopkinsHospitalinBaltimore,Maryland. In 1996,Hopkinsreported on outcomes of 3 initial cases. They concluded that laparoscopic live donor nephrectomy may be an alternative surgical modality to conventional open nephrectomy. Benefits include less postoperative pain, shorter hospital stay, quicker return to normal activities, and better cosmetic results. Other articles have supported these findings. Ratner LE, Ciseck LJ, Moore RG, Cigarro FG, Kaufman HS, Kavoussi LR. Laparoscopic live donor nephrectomy. Transplantation. 1995 Nov 15;60(9):1047-9. Bartlett ST, Schweitzer EJ. Laparoscopic Living Donor Nephrectomy for Kidney Donation. Dial Transpl. 1999:28(6):381-331. Lee BR, Chow GK, Ratner LE, Kavoussi LR. Laparoscopic live donor nephrectomy: outcomes equivalent to opensurgery. J Endourol. 2000 Dec;14(10):811-9; discussion 819-20. ____________________________________________________________________ Merlin TL, Scott DF, Roa MN, Wall DR, Francis DM, Brigdewater FH, Maddern GJ. The safety and efficacy of laparoscopic live donor nephrectomy: Transplantation. 2000 Dec 27;70(12):1659-66. In 2000, Merlin et. al conducted a systemic review of the medical literature to compare the safety and efficacy of laparoscopic live donor nephrectomy with the “gold standard” of open live donor nephrectomy. They concluded that the evidence-base for laparoscopic nephrectomy was inadequate to make safety and efficacy recommendations. Limited low level evidence suggested that the laparoscopic approach might be advantageous regarding the donor’s hospital stay, convalescence, pain, and resumption of employment. Their review found no deaths in any of the articles. Complications included hemorrhage and blood transfusions, vascular injuries, incisional hernia, bowel obstruction, and pneumonia. No statistically significant differences in donor mortality or complication rates were found comparing laparoscopic approach to the open procedure. The authors noted that this technique is still in the process of evolving. It will take “another decade or more to be confident of the risk following laparoscopic transperitoneal live donor nephrectomy.” Clinical recommendations: 1. Laparoscopic live donor nephrectomy should only be done in units where the surgeons have considerable expertise in open live donor nephrectomy. 2. The live donor nephrectomy surgical team should include a surgeon with established experience in a range of laparoscopic procedures. 3. Should be done initially in animal models or in a patient requiring a nephrectomy for benign disease (technically more difficult to recover living donor kidney since need to secure ureter and piece of renal artery/vein) 4. Transplant units should plan to do a series of these cases and maintain detailed records on cost, morbidity, and outcome of both open and laparoscopic approach. 5. Surgeons should be alert to the literature on the evolving techniques of laparoscopic nephrectomy. Of interest is the option of extraperitoneal approach instead of transperitoneal approach. Recommend: cautious introduction of laparoscopic live donor nephrectomy Studies with better quality and design, larger sample size are required. Randomized, controlled trials difficult due to ethical concerns. Best option would be several multi-center, prospective studies of large sample size and with concurrent controls. ________________________________________________________________________ Chan DY, Fasbrizio MD, Ratner LE, Kavoussi LR. Complications of laparoscopic live donor nephrectomy : the first 175 cases. Transplant Proc. 2000 Jun;32(4):78. In the first 175 laparoscopic renal harvest procedures at Johns Hopkins, the complication rate was 14%, the rate of open conversion was 2%, and 3% of the patients required transfusions. These rates improved with experience. There was no significant difference in the performance of the allografts. The most critical and hazardous part of the surgery is dissection of the renal artery and vein. Wider acceptance of laparoscopic nephrectomy will increase the number of donors and help develop methods & devices to shorten the learning curve. With any new procedure, there is concern regarding potential complications and the time needed to develop familiarity and skills. Complication rates of laparoscopic and open are similar. Complications included: Bleeding requiring transfusion Stapler malfunction Epigastric artery injury Bowel injury Pneumonia Incisional hernia Wound infection Prolonged ileus.
“Upon removal of the catheter, it was immediately apparent that attempts to free the circular spine of the mapping catheter had disrupted the mitral valve apparatus, resulting in acute mitral insuf. ciency in our patient.” __________________ On Thu, Apr 29, 2010 at 8:54 AM, Dan Walter wrote: From defendant’s pretrial statement to the Court: “Plaintiff has posted a 24-chapter ‘book’ on the Internet entitled “Adventures in Cardiology” which recounts in an inaccurate and prejudicial manner the events giving rise to this lawsuit. This is accessible to the general public and the Baltimore City jury pool and must be taken down from the Internet immediately and throughout the trial of this case.” Trial to start May 3rd. ***
- If a resident or other physician is to perform the operation under the guidance of the surgeon, it is necessary to make a full disclosure of this fact to the patient, and this should be evidenced by an appropriate statement contained in the consent. If the surgeon employed merely assists the resident or other physician in performing the operation, it is the resident or other physician who becomes the operating surgeon. If the patient is not informed as to the identity of the operating surgeon, the situation is “ghost surgery.” Judicial Council of the American Medical Ass’n, Op. 8.12 (1982). http://biotech.law.lsu.edu/books/lbb/x955.htm
————— However, prenatal dex is routinely given outside the research setting, as an off-label treatment. It is common — and perfectly legal — for doctors to use their own discretion when prescribing drugs off-label. Antiseizure drugs like topiramate are commonly prescribed to treat migraine headache pain, for example. The practice allows patients to receive valuable treatment for which the drug may not have been expressly approved and may never be — it takes money and drug-company interest, which are hard to come by, to conduct the large randomized controlled trials required for a new-use the Food and Drug Administration (FDA) approval of a drug that is already on the market. But as doctors share information about a drug’s perceived off-label benefits and lack of harm, it gets even harder to take a step back and launch a formal randomized controlled trial — considered the gold standard in medical research — because patients demand the treatment, and doctors say it would be unethical to withhold it from them or from control groups in clinical trials. “It’s a risky and dangerous way to innovate,” says prominent University of Pennsylvania bioethicist Arthur Caplan. “There’s no systematic collection of information. So, yes, things do get proven this way, and it is a way to innovate, but it also can come at a cost of unnecessary expense and, sometimes, bad side effects.” It also enables doctors to do human research without gaining proper approval. All participants in human medical research are, by law, entitled to the protective oversight of an institutional review board (IRB), a committee that safeguards the interests of research volunteers and ensures they have been fully informed about the potential risks and benefits of an experimental treatment. If doctors are simply treating a patient with an off-label drug, they are not required to obtain written informed consent from patients. But if doctors give treatment with the intent to gain knowledge, they are technically doing research, which must receive IRB approval. ____________ Congestive Heart Failure After Catheter Ablation for AF. Introduction: This study sought to describe a new complication of catheter ablation for atrial fibrillation (AF): new onset congestive heart failure (CHF) after extensive ablation for AF. http://www.medscape.com/viewarticle/744948?src=nl_topic July 2011 _______________________ Kenneday Kreiger Lead dust lawsuit 9/2011 http://www.nytimes.com/2011/09/16/us/suit-accuses-baltimore-institute-of-exposing-children-to-lead.html?ref=todayspaperPRESS RELEASE
July 11, 2011, 7:00 a.m. EDT
Endosense Reports Completion of First Patient Case Utilizing Contact-Force Visualization Software, Developed in Cooperation with Siemens
GENEVA, Jul 11, 2011 (BUSINESS WIRE) — Endosense, a Swiss medical technology company, has announced completion of the first patient case utilizing prototype software that integrates the contact-force data provided by Endosense’s TactiCath(R) force-sensing ablation catheter(1) with Siemens Healthcare’s electrophysiology solutions. Performed by Dipen Shah, M.D., on June 15 at the University Hospital of Geneva, this procedure demonstrated the feasibility of the companies’ jointly developed application for use during the catheter ablation treatment of cardiac arrhythmias. The new software was designed to give electrophysiologists access to contact force information in a fluoroscopically enabled, three-dimensional anatomic heart model with X-ray based catheter tracking system.
“This new contact-force visualization software brings a valuable new sensory dimension to the catheter ablation procedure, as we can now measure, control and also virtually see in 3D the contact forces we apply as we are applying them,” said Dr. Shah. “I believe this new level of visualization will not only make the procedure more intuitive and easier for electrophysiologists to perform, but it will also allow us to improve our ablation technique in such a way that we ultimately offer safer and more effective procedures.”
Author: Murray L. (—.cpe.net.cable.rogers.com) Date: 06-29-11 17:42 Please remember that as with ANY surgery that there is risk involved and do not forget that. In making my choice and decision to wait on the list for my ablation (I hope) I chose the best hospital in the area with one of the best electrophysiologists. My wait is going to be somewhere between ten months and two years I believe until I hear otherwise, but right now I am grinding my teeth through it and will wait. I am in Ontario Canada and the care will be without charge for the most part (sorta). The downside is the wait. I would, humbly (very humbly) suggest that not only do you want to choose a top EP FIRST AND FOREMOST, you then want to choose a top facility as Hans has suggested to you. You most certainly want to ask one question straight up front in my humble opinion before making ANY decision and that is a real simple one: “Will it be YOU diddling around inside my beating heart with the cutting edge equipment in a very complex medical procedure, or will it be a medical student or understudy?”. This is where we seperate the the boys and girls from the men and women. I will not be diddled on by a student. Period. I don’t care what I must do in order for that to happen but I will not be diddled with by a student. You want reinforcement? Read “Collateral Damage” and some other literature out there and understand that when it comes time to tune up the Ferrari, you don’t want the milkman doing it for you as a favour. ________________ Many have hopes that the hybrid procedure (combining the best manual catheter ablation specialists with the best mini-maze specialists) would improve the chances for NSR for chronic Afibbers so this is bad news.http://www.afibbers.net/forum/read.php?f=9&i=7047&t=7047 Session: Catheter Ablation of Complex Left Atrial Arrhythmias Friday, May 06, 2011, 1:30 PM – 3:00 PM Presentation: AB35-3 – Hybrid Procedure (endo/epicardial) Versus Standard Manual Ablation In Patients Undergoing Ablation Of Longstanding Persistent Atrial Fibrillation: Results From A Single Center Pres. Time: Friday, May 06, 2011, 2:00 PM – 2:15 PM Location: 2003 West Methods: Twenty two consecutive patients (group 1) with long-standing persistent (LSP) AF and large left atrium (LA) (> than 5cm) underwent ablation procedure with a combined surgical closed chest epicaridal RF ablation (nContact, NC, USA) and EP trans-septal endocardial ablation (Biosense Webster, NJ, USA). This group was compared with 35 consecutive patients with similar clinical characteristics (Group 2) undergoing manual ablation. Complications and long-term procedural outcomes were compared. Results: Baseline characteristics of Group 1 (65±8 years, 89% male, BMI 31±5, LA 5.9±0.5cm) and Group 2 (64±10 years, 84% male, BMI 31±6, LA 4.8±0.8cm) were not significantly different. Compared to group 1, group 2 had longer procedure time (120±47 versus 234±68 minutes, p <0.001) and RF time (76±18 versus 85±38 minutes, p = 0.004). Mean fluoroscopic time was not different (33±13 versus 37±15 minutes, p = 0.382). One (4.5%) patient in group 1 developed cardiac tamponade compared to 1(1.6%) in group 2. In group 1, 1(4.5%) had ischemic stroke while no stroke were present in group 2. There were 3(13.6%) deaths in group 1 (one developed atrio-esophageal fistula, a second patient died of stroke, a third patients died at follow up). No deaths were reported in group 2. At 220±145 days of follow-up, 12(55%) patients in group 1 and 19(54%) patients in the manual group (log-rank p= 0.984) were arrhythmia free after a single procedure. Conclusion: Our result shows that in patients with long standing persistent atrial fibrillation and a large atrium the combined approach increases the complication rate and does not improve the outcomes —————— Medical Discounts, Inc. Low Cost, Discount Radiofrequency Catheter Ablation $1,980 total price World Class, Low Cost Discount Cheap State-of-the-Art Radiofrequency Catheter Ablation w/Lower Costs Radiofrequncy Introduction — Radiofrequency catheter ablation is a procedure that is performed to correct a disturbance in heart rhythm. A brief review of how a normal heart rhythm occurs and a description of some of the rhythm problems that are treated with this procedure will help in the understanding of radiofrequency catheter ablation. 2009 R F Ablation Surgery Cash Discount Price The price list is for India “only”. If you want prices for medical services in other countries, call toll free (800) 771-3325. R F ablation cash discount price $1,980 ——————-
Guidelines for the Management of Atrial Fibrillation: ESC: 4. Management
4.3.5.2 Left Atrial Catheter Ablation Ablation strategies have been deployed with the intention of ‘curing’ AF in several patient populations. Long-term follow-up of these patients suggests that while sinus rhythm is better preserved than with antiarrhythmic drugs, late recurrences are not uncommon.[128] The majority of studies have recruited patients with symptomatic paroxysmal AF and no or minimal structural heart disease. For the individual patient with symptomatic AF, there must be sufficient potential benefit to justify a complex ablation procedure associated with possibly severe complications. Operator experience is an important consideration when considering ablation as a treatment option. The studies cited in support of the recommendations have been almost exclusively performed by highly experienced operators and expert staff working in specialized institutions, but in clinical practice more junior and less experienced operators may be involved in many institutions. Catheter ablation is usually undertaken in patients with symptomatic paroxysmal AF that is resistant to at least one antiarrhythmic drug. This practice is supported by the results of multiple single-centre randomized studies and by multicentre prospective studies comparing antiarrhythmic drug treatment with catheter ablation, showing a significantly better rhythm outcome after ablation ( Table 18 ). In addition, meta-analyses of studies performed mostly in patients with paroxysmal AF, comparing antiarrhythmic drugs and catheter ablation, have also shown a clearly better rhythm outcome after catheter ablation.[96,131–135] However, most of these studies have included patients already resistant to antiarrhythmic drug treatment, and the follow-up was relatively short. Data on a direct comparison of antiarrhythmic drug treatment and catheter ablation as first-line therapy in patients with symptomatic paroxysmal AF are scarce,[134] but separate analyses of the efficacy of antiarrhythmic drugs and of LA catheter ablation in AF imply greater benefit from ablation.[131] However, considering the potential of AF catheter ablation to achieve rhythm control in symptomatic patients with paroxysmal AF and minimal or no heart disease, and the relative safety of the technique when performed by experienced operators, ablation may be considered as an initial therapy in selected patients (Figure 12). … For patients with either persistent AF or long-standing persistent AF, and no or minimal organic heart disease, the treatment strategies and the benefit–risk ratio of catheter ablation are less well established. Extensive and frequently repeated ablation procedures may be necessary in these patients, and it seems reasonable to recommend that they should be refractory to antiarrhythmic drug treatment before ablation is considered. Since amiodarone treatment may be associated with serious and frequent adverse effects, especially during long-term treatment, it is reasonable to consider catheter ablation as an alternative to amiodarone treatment in younger patients. … For symptomatic paroxysmal and persistent AF in patients with relevant organic heart disease, antiarrhythmic drug treatment is recommended before catheter ablation. In such patients, successful ablation is more difficult to achieve. Major symptoms should be associated with the arrhythmia to justify the procedure. Ablation of persistent and long-standing persistent AF is associated with variable but encouraging success rates, but very often requires several attempts. These procedures are long and technically challenging, and are associated with greater risk than PV isolation alone. Whether amiodarone therapy or catheter ablation should be performed after failure of less toxic antiarrhythmic drug treatment should be carefully evaluated in individual patients. Among other factors, patient age, type and severity of organic heart disease, LA size, co-morbidities, and patient preference should be considered. There is evidence that patients with AF-related co-morbidity may gain from a primary ablation strategy; for example, patients with heart failure benefit from LA ablation as the ejection fraction and functional endpoints such as exercise tolerance may improve significantly.[93,94] The benefit of AF ablation has not been demonstrated in asymptomatic patients. http://www.medscape.com/viewarticle/730434_4_ Complications: Stenosis up to 10% for focal PV ablation. http://img.medscape.com/article/730/434/730434-tab17.jpg__________________
About AFIB Alliance
http://www.atrialfibrillation.com/medical-prof/afib-alliance Biosense Webster does not only deliver innovative, high-quality products, but also helps you develop your skills in and knowledge of the diagnosis and treatment of Atrial Fibrillation. A range of services – based on extensive knowledge and practical education – is made available to you and your EP team. The AFIB ALLIANCESM is a unique membership program designed to help you develop your Atrial Fibrillation practice. One of its primary objectives is to facilitate the sharing of knowledge and fostering of communication about Atrial Fibrillation in order to achieve the continuous advancement of its diagnosis and treatment. Should you need further information about any of the educational materials or activities mentioned on this site, please don’t hesitate to contact Biosense Webster direct. Either send your query by e-mail using the contact form provided, or use the Locations listto find your nearest Biosense Webster office. With the Afib Alliance, Biosense Webster demonstrates its commitment to the advancement of knowledge about Atrial Fibrillation. The Afib Alliance is a membership program directed towards both physicians and patients and is founded on four cornerstones:
____________
Advanced Training Course for Ablation of Atrial Fibrillation
General Info Dates 2010: TBA Location: Bordeaux, France Venue: Hôpital du Haut Lévêque Course DirectorProf. M. Haïssaguerre | Dr. Isabelle Nault This two-day course presents theoretical, practical and clinical concepts in the treatment of paroxysmal, chronic and recurrent Atrial Fibrillation. Along with case observations there are in-depth discussions on the clinical observation and significance of pulmonary vein signals. _________ LOCA LISA shake out trial 2007 v Lasso 2515 Authors cite Calkins as saying tough procedure. Radio-frequency isolation of pulmonary veins is a technically complicated and time-consuming procedure which often requires a long fluoroscopy time [4, 5]. Technological development enabled new electrophysiological systems to be systematically introduced, and made the ablation safer and the procedural and fluoroscopy times shorter. One of these systems is LocaLisa (Medtronic EP Systems, Minneapolis, MN, USA). The aim of the study was to compare the efficacy of the LocaLisa system with the conventional mapping/ablation approach to RF ablation of AF. http://www.kardiologiapolska.pl/artykul.phtml?id=65&indeks_art=1624&VSID=rszfprzc 4. Calkins H, Brugada J, Packer DL, et al. HRS/EHRA/ECAS expert Consensus Statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on catheter and surgical ablation of atrial fibrillation. Heart Rhythm 2007 ——— Douglas P. Zipes, MD, MACC, FAHA, FHRS Salary: Heart Rhythm Society, Editor Heart Rhythm Royalty: Elsevier textbooks Consulting Fees: Medtronic Contracted Research: Medtronic
Levittown Native Tells Heart-Wrenching Stroke Story
http://levittown.patch.com/articles/levittown-native-tells-heart-wrenching-stroke-story
Andrew Graham talks about the series of strokes he suffered at 27 years old.
At 27 years of age, Graham was sitting on the couch in his parents’ house when a series of strokes occurred. The story behind this is one that could make your heart stop. “Long story short, I had surgery for a heart problem I had and I was on blood thinners because I had a clot in my heart,” Graham said. Graham was helping his friend while at school in Millersville helping change a light bulb when he was electrocuted. “It was one spring, I think it was 2009 I believe, I was changing a light bulb for somebody up at college and the electricity was still on. The metal part of the bulb was still stuck, and I went to grab it with my hand and I got electrocuted,” Graham said. What caused Graham’s stroke was a heart problem he thought was fixed, but only got worse. The result from the electrocution was something called atrial fibrillation, an abnormal heart rhythm that doesn’t pump enough blood through the body. “I didn’t think anything of it at first. I didn’t think anything of it after it either. About November or so, my heart started to beat really hard, not fast, just hard like it was beating out of my chest,” Graham said. Because of the abnormality in his heart, Graham was recommended for a heart ablation. Doctors cauterize the part of his heart that was misfiring to fix it, but that didn’t go exactly as planned. “They decided to do surgery — an ablation. They ran tubes from my groin area up through my veins, up to my heart and cauterize the part of my heart that was having difficulty. That was the most excruciating pain of my life. After that I had to lay still for 12 hours, which was the second most excruciating pain in my life,” Graham said. Graham said he thought the ablation would help, but instead he said Lancaster General botched the procedure, burning a hole through his heart and esophagus. Graham said he woke up the one morning throwing up blood. Blood was leaking out of the heart and into his body and started causing infections. He returned to the hospital and was told he would be airlifted to Johns Hopkins in Maryland. To get the holes in his heart and esophagus repaired, Graham was given an eight to 10 percent chance of surviving the surgery, but after spending a couple weeks in the hospital, Graham returned home to his couch recovering. “After the surgery, I was put on blood thinners and I had missed a couple doses,” Graham said. This is what caused what he was told to be a series of strokes because not enough blood was being pumped to his head. “The next thing I remember, was waking up in the hospital. I was told I had lost my memory of, I think, the past 3 years. It was like those three years had never happened,” Graham said. It had taken him a while to recover and regain his memory, but there are a few lingering effects. “Depending on who you ask, I do and do not have lingering effects. If you ask the lawyers then, ‘No, I have completely recovered,’” Graham said. “If you ask me, ‘Yes, I do.’ When I get depressed, I get like really depressed. But when I get happy, it’s the same way; I get really happy. Sometimes when I eat, I’ll throw it back up.” Despite all his hardships, Graham said there is a silver lining. “The most important thing, with the surgery and mainly the series of strokes, I’m just happy that I can sit here and live to tell you about it,” Graham said. ___________________________________ http://www.healthcanal.com/blood-heart-circulation/17990-Landmark-Study-Catheter-Treatment-for-Atrial-Fibrillation.html MAYWOOD, Ill. — Loyola University Medical Center is enrolling patients in a major clinical trial of treatments for a common heart rhythm disorder called atrial fibrillation (A-fib). The study is comparing traditional drug therapy with a newer treatment called catheter ablation. Standard drug therapy has been available for more than 30 years. It includes drugs to prevent the heart rate from going too fast and drugs to stop the abnormal heart rhythm. But medications don’t always work, and they can cause side effects that significantly impair patients’ quality of life. Moreover, medications do not halt the underlying progression of the disease. In the newer ablation procedure, an electrophysiologist destroys areas of heart tissue that are responsible for the erratic electrical signals. A catheter (thin flexible tube) is guided through blood vessels to the heart. The tip of the catheter delivers radiofrequency energy that heats and destroys tissue. Loyola is participating in an international, multi-center trial called CABANA (Catheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation Trial). The study will enroll 3,000 A-fib patients. Half will be randomly assigned to receive drug therapy and half will receive ablation. http://www2.godanriver.com/news/2011/jun/12/duke-physicals-add-cardiovascular-services-danvill-ar-1100604/#comment_form
Catheter ablation for afib is a risky and ineffective procedure. On the same Google News page that I found this story, there is one from Levittown, Long Island: “Graham said he thought the ablation would help, but instead he said Lancaster General botched the procedure, burning a hole through his heart and esophagus. Graham said he woke up the one morning throwing up blood. Blood was leaking out of the heart and into his body and started causing infections. He returned to the hospital and was told he would be airlifted to Johns Hopkins in Maryland. The irony is that Johns Hopkins nearly killed my wife with an ablation procedure: http://collateral-damage.net
________________________________________ SAN FRANCISCO – Declaring a patient ‘cured’ of atrial fibrillation on the basis of a lack of symptoms following atrial fibrillation ablation is definitely jumping the gun, the DISCERN AF study indicates. http://www.internalmedicinenews.com/news/cardiovascular-disease/single-article/asymptomatic-af-increases-after-ablation/3856352ab6.html —-Asymptomatic AF Recurrence Clouds Perception of Ablation: As for procedural success observed in DISCERN-AF, 58% of patients postablation were free of AF lasting more than two minutes if symptoms were the guide, but the rate dropped to 46% with ILR, “indicating that about 12% of patients had asymptomatic recurrence only,” explained Verma. http://www.medscape.com/viewarticle/742497?src=nl_topicHugh Calkins 5/5/2011:
And complication rates are dropping. In the last eight years at Hopkins, he said, the complication rate has fallen from about 12% to 1.6%, which is consistent with other EP labs. Despite all the positive aspects of catheter ablation for atrial fibrillation, there are still some gaps in knowledge, he said. Not enough is known about the safety and efficacy of the procedure in the elderly, those with heart failure, and those with long-standing persistent atrial fibrillation. “These cohorts are poorly represented in the prospective randomized trials,” he said http://www.medpagetoday.com/MeetingCoverage/HRS/26303#rate
 |
|
| The Implications of Physician Tag and Release | |
| By: Dr. Wes | April 24, 2011 | |
Recently, a disturbing trend of monitoring physician quality and accountability has taken another ominous turn: tracking physicians’ movements at scientific conferences (so called “tag and release”) using RFID tags imbedded in attendees’ name badges at national scientific sessions. I have had personal experience with this at the recent American College of Cardiology meeting, and this technology will also be imbedded in the name badges for attendees at the upcoming Heart Rhythm Society meeting to be held in San Francisco in May. On first blush, it shouldn’t be such a big deal, right? It was all just a great way for companies to obtain, for a fee, the names and institutions of people who visited their display booths and for the conference organizers to track the movements of attendees. (Heck, maybe they can partner with an industry sponsor to pick up our traffic tolls on the way to the conference hall or arrange other exciting activities for us! [Said tongue-in-cheek, of course]) |
http://www.medpagetoday.com/blogs.cfm#ayk
***
“we don’t use our people as guinea pigs in the US.”
Last month, FDA device chief Jeff Shuren committed a diplomatic faux pas. While speaking with reporters about varying approval standards and safety issues in the US and Europe, he quoted a surgeon who supposedly said “under the EU system, the public are being used as guinea pigs.” And then he added his own two cents by saying that “we don’t use our people as guinea pigs in the US.” http://www.pharmalot.com/2011/02/ec-official-to-fda-official-whos-a-guinea-pig/
Powered by the largest news staff in Northeastern Oklahoma Visit tulsaworld.com for coverage of news, business, sports and entertainment.
Return to Story Cardiac arrhythmias may be caused by nutritional deficiencies by: SUZY COHEN Dear Pharmacist Saturday, April 16, 2011 4/17/2011 7:27:35 AM Dear Pharmacist: I have been experiencing what my cardiologist calls “benign” arrhythmias for two years. They come and go, and I am unable to link them to any activities, foods or medicines. We’ve tried digoxin and beta blockers, which didn’t work. He says he can fix them with ablation and a pacemaker or just leave them alone for now. Sometimes they make me lightheaded and I get frightened. Do you think I should do the procedure? – S.C., Denver I feel a second opinion is in order; perhaps you need to see an “electrophysiologist” or a neurologist to get more information. The standard of care is to do ablation (which is sort of like “burning” one of the nodes in your heart) and then install a pacemaker, which forces your heart to beat in rhythm. I just bang my head trying to figure out why it isn’t the “standard of care” to determine the underlying cause of heart disease before all the invasive irreversible procedures like ablation, angioplasty, stenting and pacemakers are done. These procedures have a place and sometimes save lives, but is it ever wrong to check for imbalances of essential minerals, vitamins and amino acids? I wish that testing RBC magnesium was routinely done, because a deficiency of magnesium is a contributing factor in heart attack. It’s often used to resuscitate someone who has flatlined. Recently, I went to the cardiologist with a friend of mine who had an arrhythmia like yours. He was offered the same procedure by his cardiologist. On my recommendation, he saw a functional medicine physician who ordered a blood test (NutrEval by Genova Diagnostics) to evaluate his micronutrient status. Lo and behold, he was found to be deficient in taurine and magnesium. Both of these were purchased at the health food store along with hawthorn extract. His heart sank into a near-perfect rhythm within two weeks. I’ve posted an extended version of this article with heart-healthy nutrients to consider. To read the rest of my column, please visit my website, tulsaworld.com/dearpharmacist
glad you are pointing out an alternative to the invasive procedures pushed by interventional cardiologists. Catheter ablation for atrial fibrillation is not as safe or effective as advertised, according to the head of the EP Lab at Johns Hopkins, Dr. Hugh Calkins. It is a procedure developed at great expense by the medical device industry and they have worked hard to ensure that has become the standard of care despite it's lack of efficacy and the risks inherent in any invasive procedure. ------------------------------------------
Calkins TASER: http://bit.ly/gNoIgu a news bulletin from Taser International titled,“New Medical Research Disproves the Acidosis Theory of Liability Used in the Heston Case… some of the research it uses (or cites) was done by Hugh Calkins.
J&J Corruption:
http://www.nytimes.com/2011/04/09/business/09drug.html?ref=todayspaper Johnson & Johnson Settles Bribery Complaint for $70 Million in Fines By GARDINER HARRIS Published: April 8, 2011 WASHINGTON — A wide-ranging government investigation of corrupt overseas marketing practices by drug and device makers scored its first major victory Friday when Johnson & Johnson admitted bribing European doctors and agreed to pay $70 million in civil and criminal fines.
Group Faults the F.D.A. on Oversight of Devices
By BARRY MEIER Published: April 12, 2011 Among other issues, the Senate hearing is expected to examine the approval and marketing of a now-recalled artificial hip sold by Johnson & Johnson known as the A.S.R., or Articular Surface Replacement. An article last December in The New York Times detailed how the medical products giant continued to sell the hip despite repeated reports by physicians abroad that it was faulty. http://www.nytimes.com/2011/04/13/health/13implant.html?ref=todayspaper Cardiology Research and Practice Volume 2010 (2010), Article ID 950763, 9 pagesdoi:10.4061/2010/950763 Review Article Atrial Tachycardias Arising from Ablation of Atrial Fibrillation: A Proarrhythmic Bump or an Antiarrhythmic Turn? *******
Heart strong — Woman campaigns for atrial fibrillation awareness
Deseret News Puff Piece Feb 2011The most common fix to heart rhythm problems is a procedure called an ablation. Ablations are done by inserting a catheter into specific areas on the body that then read the heartbeat. Special machines direct energy through the catheter to small areas of the heart muscle that causes the abnormal heart rhythm. This energy can be used to disconnect the pathway of the abnormal rhythm. Ablations usually cure the problem all together. There are no incisions involved with an ablation and the patient can leave after a day or two with just a couple band-aids.
A cardiac perforation occurred during an a-fib ablation procedure. A constellation catheter was placed in the left superior pv via a transeptal approach. A biosense webster navistar catheter was being used in the left atrium. About 30 minutes into the procedure, the patient’s blood pressure dropped. Using cardiac echo, pericardial effusion was observed. Pericardiocentesis was performed, but the patient’s chest had to be opened. Patient was stabilized and taken to surgery. The constellation catheter was fully deployed and had not been moved for 15 to 30 minutes prior to the observation of the drop in blood pressure. The positioning of the constellation looked very good on fluoroscopy, and nothing unusual was observed. At the time of the drop in blood pressure, the navistar (biosense webster) catheter was being repositioned. The patient expired upon removal of life support 3 days after the procedure. The hospital concluded the boston scientific constellation catheter was not the cause of this event.
| Event Type Death Patient Outcome Death; |
| Event Description |
It was reported that during a mapping procedure, the lasso catheter became entangled in the mitral valve. While attempting to untangle the catheter, the loop separated from the shaft. During attempts to retrieve the tip, atrial perforation occurred. The perforation could not be attributed to a specific catheter. The patient underwent surgery to remove the loop section and repair the perforation of the left atrium. ——————————— the customer experienced resistance while the product was withdrawn, and it is possible that the ring electrode was caught with the edge of the sheath’s tip causing the damage on the ring. During the visual inspection of the catheter, it was noticed that the electrode ring #1 was lifted up leaving the ring electrode to have a sharp edge, indicating that an excessive force was applied. The pu margin of electrode ring #1 was damaged from the edge of the ring. The pu margins were found to be within spec. The sheath introducer was not returned. In addition, a corrective action has been opened to address and resolve this issue. Event Type Injury Patient Outcome Life Threatening; Manufacturer Narrative The product is not intended for use in the ventricles as stated in the ifu. Visual examination of the returned product shows that torsional forces applied to the spine tip through attempts to remove it from the left ventricle caused the product damage. The repeated twisting caused the spine cover to become smaller than the ring id and allowed a space between the ring, the spine cover material and its polyurethane (pu) margin on one side. The pu margin was fully intact to the spine cover material. Event Description During an atrial fibrillation procedure the lasso spine got stuck in the left ventricle. Attempts to remove the catheter from the left ventricle using some stress maneuvers were successful. When the catheter was outside of the body it was noted that the polyurethane was damaged and reporter could see a chorda tendonae that was cut from heart. Echo showed minimal mitral regurgitation. No medical intervention was required, the pt condition is ok. *****Model Number D-1220-03-S Event Type Injury Patient Outcome Life Threatening; A pulmonary vein isolation – rf ablation procedure for atrial fibrillation was successfully performed on the right superior pulmonary vein. During this case, while attempting to cannulate the left pulmonary vein using the lasso catheter, the tip of the lasso was locked onto the mitral valve apparatus. Attempts to disengage the tip by using clockwise and counter clockwise rotation did not succeed. When the rotation made the tip line up relatively straight, a gentle tug was applied to the lasso catheter. Unfortunately, the tip of the lasso catheter broke off. Intracardiac echo showed only mild mitral regurgitation. The procedure was aborted when the catheter fracture occurred. Upon removal of all catheters and sheath it was noted on the proximal end of the lasso (at the broken point) a tiny piece of mitral tissue was attached (the size of a 2mm long 2. 0 silk suture line). A surgeon was contacted for urgent surgical removal of the catheter tip from the mitral valve. The patient was hemodynamically stable and did not report any symptoms. The surgery was successful. The patient has since been discharged to home in good condition. Manufacturer Narrative Visual examination of the returned lasso product shows the severed spring tip and the residual cardiac mitral tissue retained on the product appeared to have been twisted as evidenced by the corkscrew appearance of the tissue fragment, and the helical shape at the proximal base of the severed spring tip. Torsional forces applied to the spring tip “niti” joint, through attempts to free it from the mitral valve caused the failure. The complaint condition of no signal was confirmed. Visual examination of the product shows that the internal stiffener is not located correctly between the shaft and lumen. The shaft and lumen will not completely separate as the internal safety and puller wire hold the unit together. ____________________________ Caught in Mitral Valve: 2/6/2001 http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=320045 3/25/02 PAM http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=389357 1/2003 (Tricuspid) http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=444706 11/2003 http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=503581 11/03 http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=502076 7/2005 http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=621234 8/2005 http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=638231 6/2005 http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=642571 http://www.wasatchcardiology.com/ Dr. David Rawling, Utah Plaqintff expert informed consent ****************************************************** Patient Stories
____________I had an ablation over 3 months ago and have had a cough from the time I got out of surgery until now. I have pericarditis without effusion and have to sleep propped up. They said that the machine blew a fuse when they were working on me and they had to wait 25 minutes until the janitor could replace it. My concerns are that they would not have any imaging system after the blown fuse, and could not see where the catheter was. I think the catheter may take a while to cool, so I’m worried that it might have burned something it shouldn’t have. My heart rate jumped 20 to 25 bpm (to 100) after the procedure and it was unsuccessful. I still get Afib up to 180 bpm. http://www.medhelp.org/posts/Heart-Disease/Chest-pain-following-ablation/show/10257 ———————————- Lynn: http://www.afibbers.net/forum/read.php?f=8&i=18218&t=18165#reply_18218
I wasn’t sure whether to post this or not. If it will help someone make what I consider to be a life altering decision then so be it. I did write to Hans first to make sure that this information is something appropriate to post in this forum. Please understand that I will not talk about where this procedure was performed or who performed it. It really doesn’t matter. The EP is considered “the” electrical guy in our immediate area. Somewhat legendary even. My goal is to make sure that everyone who suffers through A-fib understands that ablation is a serious procedure not to be taken lightly. It is not a cure-all and it certainly isn’t (as we were led to believe) a “simple” procedure that you don’t even have to stay overnight for. We didn’t even know that blood thinners are needed afterwards – such was the lack of knowledge that was shared with us. I certainly do wish I had done more research as I’ve learned so much in the last six months. Let me begin by saying that my husband of 21 years died in early October. He suffered multiple complications during cardiac ablation and was left essentially brain dead. He lived for 8 agonizing days during which I was forced to make unspeakable decisions including removing him from life support. He was an athlete who completed multiple Ironman Triathlons and was in amazing physical shape. We suffered with atrial fibrillation for the last 6 years. I say we suffered because each of you know that this is a condition that affects everyone in the family. We never knew when he would have what he called “episodes”. It was difficult to make plans and many times things had to be cancelled or rescheduled. Through it all, he amazingly maintained a positive attitude. It was nearly impossible to keep him down for long – he was incredibly stubborn. He had a huge heart (no pun intended) and he was willing to help anyone who needed it. It was really apparent after he was gone how many lives he touched in his short time. I loved him dearly and have a hole in my own heart that will likely never heal completely. Because you are here, you obviously have done extensive research. Again, please do not take the ablation procedures lightly. It is surgery and there are many things that can go wrong. I am not attempting to scare anyone, but just to inform. The risks are real and they do sometimes happen to people you wouldn’t even imagine would have problems. Do not let anyone tell you that you are young and healthy and so your risk is low. Find a center that has great statistics and make them show you those stats. I do know that I am probably “preaching to the choir”. Please do me a favor and if you decide on this procedure, hold your loved ones tight. Make sure your house is in order because this is a very serious undertaking.
———————– The procedure was performed on a 50 uear-old man and the family was initially told by the surgeon that the surgery went well. While recovering in his room the patient went into cardiac arrest and a code blue was called. Despite resuscitative efforts the patient was unable to breathe for about twenty minutes and a CT scan showed that because of the prolonged deprivation of oxygen the patient suffered profound irreversible brain injury. Nurses failed to monitor the patient after the procedure and the patient’s pericardial sac filled with blood and stopped the heart from beating. As a result of deprivation of oxygen to the brain the patient was immediately placed on a respirator and remained unresponsive. The patient died shortly thereafter. http://www.erlegal.com/lawyer-attorney-1494804.html _____________ the doctor put the catheder up through my groin and into my left (i think) heart valve. When he put the catheder in through the valve the catheder became tangled on one of the chordae that helps hold the valve shut. The doctor tried to get the catheder untangled and ended up damaging/tearing one of the chordae on that valve. The doctor told my parents that they were sending the catheder out to “engineering” to find out if there was something wrong with it because they have never had this happen before in all of the heart ablations that they have done. The doctor said it was probably just because my anatomy was different and he really couldnt explain why this happened. I dont have health insurance because im 24 and never thought that i would have heart problems at this age and i was going to pay for this ablation myself with my own money. Well now that this is happened i will have to pay for the ablation that they didnt do because they had to stop and ill have to pay for being in the hospital for longer. Then, ill have to go back and get the ablation done a 2nd time AND get my heart valve fixed. http://forums.wrongdiagnosis.com/showthread.php?t=8584 —————
http://www.medhelp.org/posts/Heart-Rhythm/Pulmonary-Vein-Ablation-Complications/show/339578?personal_page_id=332131#post_2058195 i am a 35 year old male who was on the VERY active side 6 months ago. I had an episode of A-Fib while playing basketball and in the ambulance my pulse was irregular and at 300. It was diagnosed as atrial fib with a high ventricular response. My cardiologist recommended ablation. I had my ablation on June 21st. Since then, I have never really felt “good”. Over the past 4 months, I was noticeably getting more fatigued and short of breath. A month ago, I was diagnosed with double pneumonia and was given Levaquin, 2 Z-Packs, and 3 shots of Rocephen. Nothing changed. As a result of a right heart cath. study, and later a Pulmonary CT, I have now been diagnosed as having 2 pulmonary veins with severe stenosis and one with mild to moderate stenosis. I also have a bit of fluid in my lungs. I am currently waiting to hear from the Mayo Clinic in Rochester, MN so they can do a pulmonary vein angio/stent procedure. Have any of you heard of this complication? I have not really heard anything regarding my future prognosis yet…any clues? Needless to say, I have never been more physically and mentally down in my life!
Lasso Catheter entrapment 2010: http://europace.oxfordjournals.org/content/early/2010/10/05/europace.euq309.abstract Cardima Timeline July 1997 IDE approved Pathfinder Micro for AF mapping July 9, 1997 Two patients treated in beginning of Mapping Feasibility Study* excerpts toward the bottom of this page http://www.accessdata.fda.gov/cdrh_docs/pdf/K971975.pdf July 1998 IDE approved for Pathfinder for diagnosis of VTac (mapping) April 3, 1998– Berger feasibility study Pathfinder Ablation “the first patient in its (AF) ablation feasibility study was successfully treated last week.” 1998/99 Calkins Dog Studies Nov ’98 AHA Dallas: Ruskin announces Calkins dogs studies and Principal Investigator Dr. Jeremy Ruskin highlighted results from the recently completed AF feasibility ablation study in the United States consisting of 10 patients from Massachusetts General Hospital…. What study is this?Is it Berger with the Pathfinder?
According to Progress in catheter ablation: clinical application of new mapping … REVELATION was used in all ten patients
Feb 1, 2001431 Jan 31, 2001462 Dec 20, 2000327
Cardima Receives $8 Million From Medtronic for Certain Patents.Cardima receives $8 million from Medtronic for intravascular sensing and catheter patents. Dec 1, 2000
| Cardima to Hold Fourth Quarter and Year-end Results Conference Call February 7. |
| Cardima Receives $4 Million Payment From Medtronic for Intellectual Property Sale. |
Dec 19, 2000 Contract to sell patents to Medtronic
William N. Starling Cardiac Pathways SUNNYVALE, Calif.--(BUSINESS WIRE)--June 13, 1996--Cardiac Pathways Corp. announced today that it has made an initial public offering of 2,500,000 shares of Common Stock at a price of $19 per share.
—————————- 2001 India Oral Cancer http://www.circare.org/im/im13Aug2002.htm
==================== 2002 Informed Consent Estrogen study http://www.hhs.gov/ohrp/detrm_letrs/YR02/apr02y.pdf
FDA Stent Experts Have Financial Ties to J&J, Rivals (Update2) Dec. 4 (Bloomberg) — Six physicians with financial ties to Johnson & Johnson and other heart-device makers will be advising U.S. regulators whether to restrict the use of some products because of potentially lethal side effects. ***** In other words, what was ‘on label’ for doctors was ‘off label’ for manufacturers. The FDA has put additional pressure on companies in order to encourage new approvals specifically for treating AF. http://www.fredlaw.com/bios/attorneys/klepinskirobert/Klepinski_JMDRMay2009.pdf On July 30, 2008, the Centers for Medicare and Medicaid Services (CMS) released a proposed list of topics for potential National Coverage Determinations (NCD)for public comment. The list, which will be released quarterly, includes catheter ablation for treatment of atrial fibrillation. CMS is seeking public comment on the following:
“Ablation for atrial fibrillation: If medication is not effective or not tolerated for atrial fibrillation, a non-surgical procedure called catheter ablation may be chosen. Focal and circumferential catheter ablation for atrial fibrillation is still being studied in investigational trials but may be done in selected patients to try to cure atrial fibrillation. Is the evidence adequate to demonstrate health benefits in the patients who receive the procedure? “
November 25, 2008 An FDA panel unanimously recommended approval of an A-Fib Ablation Catheter, the first to be so recommended. (Up to this point doctors had been using ablation catheters off-label.) http://www.theheart.org/viewArticle.do?primary Key=923617 (As a consequence of this FDA panel decision, Pulmonary Vein Ablation (Isolation) procedures have officially entered mainstream medicine and can no longer be considered “experimental.”) ***** William Laskey on Ethics:”There are many areas in which there can be a conflict between the patient’s best interest and the physician’s own personal interest…. The economic impact of invasive and interventional cardiology has led to pressures from several directions. Seeking increased revenues, hospitals and departments of medicine exert pressure on cardiologists for more procedures and higher fees. National and state credentialing standards for minimal procedural volumes (and the publication of individual statistics in some states) influence cardiologists in case selection, especially low-risk cases. Their economic productivity and the inherent risks of the nonsurgical procedures they perform have exposed them to increasing litigation and rising malpractice premiums. Competition for technology creates an incentive to participate in clinical research, often sponsored by industry, another potential source of revenue for individuals, departments, and hospitals. The sponsorship by industry of both formal and informal educational seminars presents potential ethical conflicts to both invited lecturers and invited audiences. As a result of these pressures, consideration of the ethical challenges for the invasive cardiologist is of timely and vital importance…. The patient has a right to be fully informed not only about the procedure being planned but also who specifically will be performing the procedure. If a fellow-intraining will play a major role in the procedure or if physician extenders are used, their roles and responsibilities should be explained to the patient. No matter what roles others play, the attending cardiologist is still responsible for every aspect of the procedure. (PDF in mydocs) ******** William Starling: Synergy, Synecor: http://www.synergylsp.com/SynegyPR_01-08-08.pdf ***** ****2006 Symposium Calkins Fistulas, silent afib etc: http://www.a-fib.com/BostonA-FibSymposium2006.htm ***** Atricure DOJ Relator’s comment 2/2/2010:http://www.thestreet.com/story/10672931/1/relators-attorneys-comment-on-atricuredoj-settlement.html”The misuse of medical devices has the potential of exposing patients to dangerous procedures and taxpayers to payment for unwarranted claims against Medicare,” said Tim Johnson, United States Attorney for the Southern District of Texas. “This settlement demonstrates the government’s commitment to maintaining safe and affordable health care for its citizens.” ** Barry Meier NYT Sept, 2009: At Medtronic, a Profit Goal for Training Inquiry Into Medtronic’s Marketing NYT March 2009 In a regulatory filing on Wednesday, Medtronic said it received a letter Feb. 9 from the Justice Department announcing a government investigation into promotion of cardiac ablation therapy. The company, based in Minneapolis, said it would comply with the inquiry. Medtronic, Johnson & Johnson, the Boston Scientific Corporation and other makers of medical devices have said they plan to enter the ablation market, in which devices are threaded through tubes in the circulatory system to burn, freeze or otherwise kill rogue heart cells. *****
∞
The results of the investigational procedure for the first 75 patients was pretty disappointing: a 52% success rate and complications galore: “When you think about complications, they were memorable, two strokes, three tamponades, the mitral valve Lassoed, an occluded pulmonary vein, some vascular complications… so I didn’t feel this was the answer—at least for the patients that I had to deal with, and deal with the aftermath.” The Lassoed mitral valve, of course, belong to Pam. She and 74 other people underwent a technically challenging high-risk procedure performed by a trainee to learn whether a theory should be put into practice — and the answer was no. The next group of 75 patients was treated with the circumferential method and the results of that investigation were even worse, 35% success rate and a 7% complication rate. It turned out that what seemed to produce the best short-term results was the hybrid approach, the combination of the two procedures. Still, there was no telling how well any of these procedures worked in the long run.
At a later venue, he tossed off some anecdotes about patients who paid the price for his ability to “do whatever he pleased” in Room One at the Hopkins EP Lab. “One of the problems was pulmonary vein stenosis. A typical case is someone who had pulmonary vein ablation shows up in the ER with three pulmonary veins completely blocked and the fourth one 90% blocked. The patient gets emergency heart surgery and dies. Another person gets an Afib ablation, you get a call, the patient has been diagnosed with lung cancer, well it wasn’t lung cancer, it was an occluded pulmonary vein that appeared to be lung cancer, but the patient got a lung removed. There was this iatrogenic epidemic of pulmonary vein stenosis… So, a 52% success rate, 6% complication rate, four deaths, so on and so forth …” So on and so forth. That’s just how the EP cookie crumbles. “When I talked to my colleagues, they said well this problem of collateral damage happens everywhere, and all of us have to think about collateral damage… I learned a lot of things the hard way… for persistent or permanent Afib this procedure is just awful—a 20% success rate. Complications in the study we did, they were memorable. Three strokes, three tamponades, the mitral valve lassoed, pulmonary vein stenosis, some vascular complications.” Calkins later said that the numbers were so bad from the study that his partner Ron Berger told him not to publish it, saying “We’d never get anymore afib patients.” They decided to find a successful subset of patients for whom the procedure seem to have some effect and lead the article with that. “And now there’s a new complication, gastric hypomotility and pyloric spasm, reported by Dipen Shah. He had four ablation patients who presented within a week with this terrible bloating of their stomach, vomiting and so forth and they literally had this paralyzed stomach. One patient had to have a gastric bypass or something horrific… “So it’s just another risk to put on the consent form.” **** Web-based tool makes cardiac procedure risks more transparent: http://www.cardiovascularbusiness.com/index.php?option=com_articles&view=article&id=22239&division=cvb&division=cvb ****** “Catheter ablation of atrial fibrillation reduces the risk of Alzheimer’s disease and dementia” http://intermountainhealthcare.org/hospitals/imed/about/news/Pages/home.aspx?NewsID=383 http://www.theheart.org/article/1079365.do (READ THE COMMENTS) ******** Press Date: 11/20/2000 Riverside First to Use Lasso Catheter: http://www.ohiohealth.com/body.cfm?xyzpdqabc=0&id=384&action=detail&ref=11 ” With the LASSO, the expected success rate is about 70 percent. Our long term goal is to cure AF rather than to just treat it… Co-invented by Dr. Michel Haissaguerre, Professor, Hôpital Cardiologique du Haut-Lévêque, Bordeaux, France, and developed by Biosense Webster (a member of the Johnson & Johnson family of companies marketing healthcare products), the LASSO is the first circular catheter capable of circumferentially mapping pulmonary veins. It received 510(k) market clearance from the U.S. Food and Drug Administration (FDA) for atrial mapping two weeks ago…” ***** Dr. John M: “Dabbling,” in AF ablation is a “real-world” problem.: http://drjohnm.blogspot.com/2010/05/dabbling-in-ablation-is-not-so-good.html Industry front groups: http://www.cspinet.org/new/pdf/lift_the_veil_guts_fnl.pdf******* And then in December 2003, two years after Josie King, Johns Hopkins Medicine issued this statement:
Statement from Johns Hopkins Medicine regarding the death of Brianna Cohen
With permission from the family given December 17, Johns Hopkins can now, and with deep regret, sadness and apology, publicly report and take responsibility for the untimely death December 4, 2003 of Brianna Cohen, 2, the child of Mark and Mindell Cohen of Owings Mills, Maryland. Brianna was, at the time of death a child with cancer followed by the staff at the Johns Hopkins Childrens Center. She was being treated at home with Total Parenteral Nutrition (TPN) through intravenous infusion services provided by Pediatrics at Home, a subsidiary of The Johns Hopkins Home Care Group, when her parents found her unresponsive and took her immediately to the nearest community hospital, where she was pronounced dead
******* http://tinyurl.com/dayincourt ******************** Ironically, her catchphrase was “Is it fair to say then that …” Then go on to distort some facts. So is it fair to say then, that …. http://heartheaded.wordpress.com/ **** http://robertsfight.wordpress.com/ ****** Science for Sale: http://psychrights.org/Research/Digest/Science4Sale/Science4Sale.htm April 19 (Bloomberg) — Hospitals rated as top by U.S. News & World Report are chosen using a system that reflects their reputation with little connection to objective measures of quality of care, a study said. ******* Calkins Dog studies 2000: “Although the feasibility of curing atrial fibrillation with catheter ablation techniques has been demonstrated using standard catheter ablation techniques, the procedure is extremely time consuming and associated with a high risk of complications. For this reason there is general agreement that new type of ablation systems, designed specifically to create continuous linear lesions are needed… A learning curve was observed during these procedures. ****** On “Sorry Works”: The English author G. K. Chesterton wrote: “A stiff apology is a second insult. … The injured party does not want to be compensated because he has been wronged; he wants to be healed because he has been hurt.” _____ “There are also documented cases of under reporting but I am afraid of starting a flame war on this here. (it would make a good chapter though in your adventures blog…” researcher ______ So Calkins haltingly recites the company line: “The most critical aspects of the procedure I was performing. At the time of the… I was performing the critical aspect of the procedure, the most critical aspect of the procedure, deciding where to give the energy, how much to give, when to stop burning, and that was the aspect of of the procedure that I, as the attending physician, was doing… I was performing the most critical aspect of the procedure.” A lawyer asks if maybe corkscrewing a catheter into the left ventricle might be considered a critical aspect of the procedure. “Same complication could’ve happened if I was going to play with the catheter. I have no reason to believe that was something attributable to Dr. Wu versus myself manipulating the catheter. It’s something inherent in having the catheter in the heart.” This from a guy who professed quite a bit of surprise when it did happen. Whether or not Hugh Calkins had any reason to believe that he, a twenty year veteran, would not have made the rookie mistake of turning the catheter knob the wrong way, he had no right to deceive my wife about who would be playing with the catheter in the first place. ****** Dr. Calkins was on a quest to cure atrial fibrillation. A worthy goal. He wrote in the European Heart Journal in November, 2001, about a doctor in France had treated three patients by burning scar tissue inside their hearts. The doc wrote that the ablation technique “could result in cure of atrial fibrillation.” That would be a very big achievement, There were a lot of questions to be answered. and a lot of problems to be overcome. They didn’t know exactly where in the heart to burn these scars and they did not know which tools were the best to use. They thought they had a pretty good idea of what needed to be done inside the heart to stop people from having afib. But they didn’t know for sure if it worked and they didn’t know the best way to go about getting the job done. Despite a promising paper from a doctor in France who treated three patients, they did not know if the procedure was safe or effective. Dr. Berger has said the he and Dr. Calkins did a lot of research on people up at Hopkins trying to find the answer. As of 2007, Dr. Calkins still didn’t know if the procedure worked in the long run. And, in his words, he “learned a lot of lessons the hard way.” The only way to see if the procedure was safe or if it was to try it out on people. Research. On people. And they would have to learn by trial and error. ***** ∞ Lecture with slides Hugh Calkins discussing Vasemreddy study. Thursday, May 18, 2006 7:00 PM � 10:00 PM Westin Copley Place, Boston, MA Video:http://www.vindicomeded.com/cmelc/tc_lecture.asp?rid=17208 Brochure: http://cme.cybersessions.org/HRSdinnersympo/ “So what I would like to do over the next 15 or 20 minutes is go over of at least my perspective of catheter ablation for atrial fibrillation, we’ll talk about where we are now. We’ll talk about the current approach, what we use today, some future directions and then conclusion. You know catheter ablation for atrial fibrillation really came to life in 1998 when Michell Hassaguere published his paper in the New England Journal of Medicine talking about the pulmonary veins as a trigger for atrial fibrillation. And in that paper he had this figure which is really remarkable it shows the onset of atrial fibrillation arising from the pulmonary vein so you can see you have a beat of sinus rhythm, atrial fibrillation. This is a catheter in the right inferior pulmonary vein you have an atrial potential and this very tall potential is a pulmonary vein potential and then you’ll notice that when the atrial fibrillation starts, the pulmonary vein potential drives the atrial fibrillation. The atrial fibrillation is in fact emanating from the pulmonary vein. So in this paper they identified the pulmonary veins as the common source of atrial fibrillation. More commonly the superior than the inferior pulmonary veins and they had quite good success. So the concept is, you have these pulmonary veins enveloped in muscle sleeves, you have a trigger of focal firing in the pulmonary vein. That in turn acts like the starter on an engine, it gets the atrial fibrillation going and then the atrial fibrillation will sustain in susceptible patients and this was really a very novel idea to what all of us had learned in medical school. And then to get rid of atrial fibrillation you go in, you find the spot and you ablate the site. Now the problem with that approach was this, was pulmonary vein stenosis. So here’s a pulmonary vein before ablation here’s one after ablation you can see one over here the tremendous pulmonary vein stenosis. So in those early days electrophysiologists who were well meaning trying to cure atrial fibrillation enthusiastically took off after Michelle to do this job and they ended up, you know, spending twelve, fifteen hours in the EP lab looking for these focal sites of initiation for afib they’d burn these areas, feel quite pleased with themselves, and the patient would show up with problems. And there were remarkable stories that emanated from around the world about pulmonary vein stenosis. A typical case is someone, in another country, who had a pulmonary vein ablation. The patient shows up in sort of extremis with three pulmonary veins completely occluded, one 90% occluded, of course the patient had their ablation done in another institution, the patient gets emergency heart surgery and dies. Another patient gets an afib ablation, you get a call, the patient was diagnosed with lung cancer. Well it wasn’t lung cancer, it was an occluded pulmonary vein that appeared like lung cancer and the patient got their lung resected. So this was a whole new epidemic of sort of iatrogenic pulmonary vein stenosis that well meaning electrophysiologists we unaware of… And when you talk to you colleagues – I would talk to my colleagues about this and they said “well, this problem of collateral damage happens everywhere not just in Iraq, but also everywhere in the body. So the urologist would be there ablating bladder cancer,thinking they’re getting rid of the bladder cancer, forgetting the bowel is on the other side and they wind up perforating the bowel. So all of us have to think about what other structures, what collateral damage we’re going to get. So really where I became enamored with afib ablation, with this pulmonary approach, was when the Lasso catheter was developed by the group in Bordeaux. And the idea was that you have a circular catheter in the pulmonary vein, you can then go and electrically isolate the vein, ablating outside the valve ring and basically achieve the same thing. Now I learned a lot of things the hard way about the Lasso catheter. One way, you can lasso lots of things with it, including the mitral valve and if you happen to Lasso the mitral valve it’s very hard to untangle the valve and when we tried to untangle it, we ended up ripping the valve and having to replace the valve, and so that was a memorable Lasso experience. So just keep in mind, and then of course they tell you, the lawyers tell you,well in the package instructions it says, you know, never place this near the mitral valve, well if you know where the pulmonary veins are, they’re very near the mitral valve, so it’s very hard not to lasso the valve occasionally. So anyhow, so I went ahead and started doing the procedure and these are the results that I saw in our first 75 patients. So 75 patients, most of them had paroxysmal afib, some had chronic afib. Most had one procedure, some patients had two procedures. Ten months of follow up. Fifty two percent of patients free of afib, thirteen percent improved and those with persistent or chronic afib or those over fifty did worse. And when I looked at sort of a life table analysis what we see is something like this like the longer, the more you follow the patients, the more the afib occurs. It looks rather like an anti-arrhythmic drug. Now if you read the literature you may saw ‘Well what is wrong with us'[hopkins] these patients in Baltimore, other places you get an ablation it’s a straight line, it never recurs for about fifty year, but in Baltimore, the longer you follow them, the more afib you see, and much like again anti-arrhythmic drugs. And this is just our reality. Because I’ve learned that you can read the literature but the end of the day, I really believe what I see in my own hand. and then you look at this with persistent and permanent afib, this procedure was really awful – at the end of the year you had about a 20% success rate so if someone’s been cardioverted once for afib, the segmental ablation strategy really was not very impressive. When you think about complications, they were memorable, two strokes, three tamponades, the mitral valve Lassoed, an occluded pulmonary vein, some vascular complications, and my assessment was that the results were certainly lower than the literature had said, the complications were certainly greater than the literature had said, and I didn’t feel this was the answer — at least for the patients that I had to deal with, and deal with the aftermath. If you look at sort of the published literature, you end up with about a 68% success rate for this procedure, 70% for paroxsysmal, 30%, very low for persistent or permanent, Three point six percent pulmonary vein stenosis, 0.8% stroke 0.2% tamponade. Again, somewhat consistent to our results, although our results weren’t quite this good. So then I said, ‘Well what else is there? Well another option that emerged on the scene was the idea of circumferential ablation. Instead of doing this point by point burning, let’s just go ahead and put a big Lasso, you know ablate around the whole ostial portion of the pulmonary veins. And this really came to the front when Carlo Pappone published his paper in JEC [Journal] describing a large series of patients who either had catheter ablation of afib with a circumferential approach, or drug therapy this was not a randomized study it was just what patients preferred but the results were impressive. Three – 900 days of follow up – daily event monitors. Results: Ablation reduced afib occurrence, mortality morbidity quality of life. And if you look at the curves they were really quite impressive, some early recurrence but about an eighty percent success rate with catheter ablation — much less for anti-arrhythmic therapy — so I said this really seems to be a good deal lets get out to Milano and have a visit and so I did. I went out and visited Carlo for a week and started doing the procedure. So this is one of our first procedures with that. Again you have the pulmonary veins and these are the circuling (sic) lesions. Now skeptics would say that the problem with the procedure is that the end point is a red dot on the machine. That’s really not the case, that you really want to get rid of voltage inside the ablation area. So how did we do the first 70 patients; average age of 56 years, most had chronic Afib, one procedure, six months of follow up and we had 56% of patients free without drugs, 76% Afib free with drugs, one tamponade, one stroke, two PV occlusions and early recurrence seemed to predict failure and again this is what we saw. If you had early recurrence afib in the first three months, you had a 50% success rate otherwise you ended up up with about and 80% success rate. If you look at the published literature you end up with about a 63% overall success rate, 72% for paroxysmal, 49% for persistent and permanent, 4 percent atrial flutters, .4 percent stokes, .6 percent cardiac tamponades. Now at this meeting, we have an abstract, it’s a rather famous abstract where I had a fellow come on and I said, ‘Well why don’t you look at the long term follow up of catheter ablation for atrial fibrillation. Most studies you look at the mean follow-up’s from one day to ten months or one day to two years, but very variable follow-up and I said let’s look at follow-up with a minimum of follow-up of twelve months and lets look at single procedure outcomes, meaning if you have on catheter ablation and you’re getting done again three months later, either the billables are a little down or else the patient failed the first procedure. And so we said let’s take a harsh look at our numbers and see how we really did and it was somewhat appalling. I think our success rate was about 35% for a twelve month single procedure success rate, with a 7% complication rate. And my colleague Ron Berger says, he says, well you can’t publish these data, we’ll never see another patient again at Hopkins. And I said this is the truth this is what we found, you know the fellow spent a year looking at this data, this is a heck of a message to send to our fellows not to publish it. And he said can you find a silver lining. So we did identify a subset of patients with paroxysmal afib that were young and had a small left atrium and had blue eyes and had a 70% success rate — but for the rest the success rate was much worse. So we sent the paper in to be published to the Heart Rhythm Journal and it got rejected, but I sent it in again and I said this is a really important piece of paper, but it got rejected again. So I sent it in to the Journal of Interventional EP and they took it and I sent it in to the Heart Rhythm meeting and I had sort of a mixed reaction and my fellow called all delighted and he said that ‘I just heard that I just won the Eric Prystowsky Clinical Research Prize from the Heart Rhythm Society and I said well, my goodness, fantastic, so then I went to Eric and I said what is this prize, and apparently the prize is for the top scoring clinical abstract at the meeting submitted by a fellow – anonymously – so of all of the abstract submitted, this 32% success rate abstract was number one, so there he was today at his presentation, big award and all the rest of it with these awful results. But I was reassured when some folks from Copenhagen, in a later session, presented almost identical data with their experience. So it’s not just Baltimore, it’s Baltimore and Copenhagen that seemed to have the problem with long term follow up with some of these earlier procedures. So this was an easily performed procedure. The result was certainly less than I anticipated. You can develop these left atrial flutters. Safety’s better, but we really need to do better. And then you look at Ricardo Capato put together a meta analysis… of a lot of series, or a survey and he looked at 100 centers worldwide, 9,000 patients and he ended up with a 52% success rate off drugs, 25% with drugs, 6% major complication rates, four deaths, so on and so forth. So again our results are not that different than the worldwide results when you factor in that a lot of these worldwide patients had two procedures. So what do we do now? We know have an approach we call the circumferential abltion with isolation or the Pappone Plus, or you can say it’s the Milan and Bordeaux approach combined, but I think it works quite nicely. So this is something that Carl Hienz Cook, sort of I think reported first, the idea of making the same circles that Carlo makes but the end point is a Lasso catheter, you have a more objective endpoint than the red dot or than voltage mapping by the old fashioned way and again, he had fantastic results — 76% success in a month 95% success with a reprocedure. Nine patients, but again very imrpessive and this is what we switched to and what we still do today. As you go ahead and do the procedure you can see the pulmonary vein potentials sort of merge as you make these lines. Here’s a pulmonary vein potentials markedly delayed as opposed to here and ultimately you isolate the pulmonary veins. This is just the sort of the approach we use, again big circles around the veins, you can puill in the esophagus with the mapping systems that we use now… Just another view of the right sided veins and the approach we use. So what success? Sort of the worldwide success, well this approach is really quite similar to what many centers now do, the Cleveland Clinic, some other centers, about an 83% success rate, 82% for paroxysmal afib, 50% for persistent or permanent, 1.6 for left atrial flutters, 0.8% for strokes, 0.3% for tamponades. So what’s our results now, well I can’t tell you the twelve month follow up single procedure success rate because our fellow has to get to work on that. I can just tell you my sort of gestalt by seeing these patients in clinic and my gestalt is that this is a major advance, that it’s not one technique or the other technique, when you combine them you get better results. And 70 to 80% single procedure success in the optimal patients. An optimal patient is young, has a small left atrium and paroxysmal afib. 40-70% single procedure success in others, the 76 year olds those with the big atrium with permanent afib, efficacy is clearly induced, improved, with redo procedures. There’s some risk of pulmonary vein stenosis, a small risk of cardiac tamponade, a small risk of stroke. We’ve heard about esophageal fistulas, one in a thousand. And now there’s a new complication that Dipen Shah just reported and that is gastric hypomotility and pyloric spasm. So he published a paper with four hundred patients had this procedure and four presented within a week with this terrible bloating of their stomach, and vomiting and so forth and literally had this paralyzed stomach that wasn’t contracting. With the thinking being that when you ablate in the posterior wall of the atrium you ablate these vagal fibers that run along the esophagus and you get rid of innervation to the stomach. Two of these patients apparently did well with the conservative management NG tube. One patient had to have some kind of a gastric bypass or something horrific to take care of it so again, it’s just another risk to put on the consent form. So what are the future generations there’s obviously a lot going on if you sort of look around at at the meeting, there’s a lot of excitement for new ablation technologies, cryo ablation, balloon or catheter based focused ultrasound ablation, stereotaxis, ah, laser balloons, ah, and then there’s new strategies. So this is just the cryoablation which appears to be a quite safe energy source that’s in clinical trials. This is focused ultrasound, one of the balloon based methods where you put this outside the pulmonary vein and you have forward focused ultrasound. There’s new approaches with vagal ablation that Sonny Jackman is really spearheading, the concept that if you ablate vagal ganglia within the atrium you can have a very high success rate. This is something that Carlo Pappone drew attention to initially that Sonny Jackman is now carrying forward. It looks very promising but again has not been replicated by other centers. I think we have to say that it’s promising, but clearly investigational. Rianamami (ph) has a cafe’ approach where you ablate rapid fractionated areas in the atrium. Completely different strategy he reports very good success rates, but agian early data, no multicenter data and not confirmed by other institutions. So let me just conclude that circumferential ablation with PV isolation appears to be a safe and relatively expeditious approach to the treatment of patients with atrial fibrillation. We now offer this procedure to patients with highly symptomatic afib refractory to at least one anti-arrhythmic drug. The best results are certainly achieved in younger patients without structural heart disease who have paroxysmal atrial fibrillation. And new technologies and approaches are being studied with hopes of further improving the safety and efficacy of catheter ablation of atrial fibrillation and determining if additional lesion sets are needed for patients with chronic atrial fibrillation. I just want to finish with a cartoon that Serge Belz (sp) brought in to me, which I think is very apt. Here’s a patient, where all that’s left is their head and their feet, and here’s the rest of him…”Have we done enough work in the left atrium to prevent atrial fibrillation?” And that’s really the challenge. With some of these approaches you really wonder if there’s an atrium myosite [muscle cell] left at the end of the procedure and we want to do as little as possible to eliminate the atrial fibrillation. So I thank you again for the invitation and it’s been a pleasure being here. In a series of 348 irrigated-tip AF ablations with complete PV isolation including LA linear ablation in 254 and cavo-tricuspid isthmus ablation in 265, 10 patients (2.9%) suffered cardiac tamponade during the procedure. All tamponade occurred during linear ablation attempting to create bidirectional conduction block in either the left or the right atrium. In eight out of 10 patients, cardiac tamponade was associated with “popping,” consistent with tissue disruption. A comparative analysis between patients with and without tamponade revealed that RF power was significantly higher in patients who developed tamponade (53 ± 4 vs 48 ± 7 W). The subsequent decision to limit power delivery to ≤42 W during linear ablation reduced the incidence of cardiac tamponade to 1% (four cardiac tamponade among the subsequent 398 procedures). A further power limitation to ≤40 W resulted in no cardiac tamponade in the next 167 AF ablations.[10] **** Kennedy Kreiger/Tuskeegee http://www.rooflines.org/1070/baltimore_what_the_nyt_didnt_see_fit_to_print**** Defacto Medical Trials at Johns Hopkins
“So Ron Berger says, ‘Well, you can’t publish these data. We’ll never see another patient again at Hopkins.'”
The brochure for a continuing medical education video course on atrial fibrillation produced by Today in Cardiologylooks like the cover for a music CD or video game. There is a warning: Unlabeled and Investigational Usage The audience is advised that this continuing medical education activity may contain references to unlabeled uses of FDA-approved products or to products not approved by the FDA for use in the United States. The faculty members have been made aware of their obligations to disclose such uses.Hugh Calkins was talking about complications and he reeled off some stories and called it collateral damage and he compared himself to a cancer surgeon who might be *****
Study group ID
“Our first 75 patients (collateral damage video)
“Here the plaintiff’s case is bolstered by speculation about why Dr. M did not provide Mr. W with the information about the senior fellow’s experience. She wanted him to have the biopsy and she wanted her senior fellow to develop experience in doing this kind of medical work, but she feared that Mr. W. would withhold his consent if she provided Mr. W with this information. That is, she knew this information would be material to this reasonable patient. Here the physician’s interest in the therapeutic value of the treatment is tempered, at least, by her independent and potentially conflicting interest in training her fellow. Where the physician has such a potential conflict of interest, it is especially important that the patient be given all of the information that he would deem important in consenting to treatment. It would hardly be surprising under these circumstances for the patient to feel defrauded if he later found out that such information was withheld. Doctor M’s actions are not so different from the “ghost surgery” that was common 25 years ago when surgeons would get consent to do surgery that would actually be performed by another surgeon who’s identity would not be revealed to the patient.
“The fact that this procedure was performed at a teaching hospital is not relevant… Patients admitted to teaching hospitals do not understand that they will be subject to the trial and error by students and any general consent to be used as a teaching prop is probably itself illegal… Finally, the responsibility to assure that a fully informed consent has been obtained falls squarely on the physician doing the procedure…”
Ward ethics: dilemmas for medical students and doctors in training By Thomasine Kimbrough Kushner, David C. Thomasma
******* http://www.kevinmd.com/blog/2010/02/treating-atrial-fibrillation-catheter-ablation-tv-ethical.html Let’s be clear: there is no evidence in the literature to support the statement of an 85-90% success rate for catheter ablation of atrial fibrillation. To present this kind of statistic to the general public, many of whom may have atrial fibrillation, or may know someone who has atrial fibrillation, is completely irresponsible. Catheter ablation is emerging as an important therapeutic option for some patients with atrial fibrillation, and it is indeed an impressive medical advance, but it comes with a lot of caveats. ***** http://www.healthnewsreview.org/blog/2010/02/whats-wrong-with-nbc-today-show.html
*****
***** JAMA NAVISTAR THERMOCOOL Study Have we overestimated the health benfits of ICD therapy: “Stacking the deck: antiarrhythmic drugs as “control” arm and beta-blocker inequity.” http://content.onlinejacc.org/cgi/content/full/52/14/1111 “With modern medicine, less emphasis has been placed on the physician-patientdialogue where concerns and expectations are freely exchanged.Physicians should understand that choosing longevity with potentialtradeoffs in device-related complications and quality of lifeis a personal decision that must be individually tailored topatient preference. The process of obtaining informed consentfrom patients mandates and pre-supposes that physicians, first,are fully informed of the risks and benefits of the therapythat they are offering. It is ethically imperative that we arehonest with the data, so that we can be honest with our patients.” ***** SHAM 2004 FDA Guidelines: “Sham controlled studies allow the sponsor to evaluate for procedure/placebo effect and to mask study subjects. This type of study design may be most appropriate for studies with subjective endpoints such as reduction in patient-reported symptoms, or when the risk level for the sham procedure is particularly low. FDA recognizes that it may be difficult for sponsors to develop a clinical study design with a sham control arm that both investigators and patients believe is ethical; for this reason, studies involving a sham control arm should be carefully designed with due consideration to risks versus benefits.” http://www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/ucm072590.htm *** Advances in Afib 2009 “The role of ablation relative to AAD for first-line treatment of AF is less clear. Only one small randomized study (67 patients) has addressed this question.30 While ablation did appear superior to drug therapy in this study, nearly all (96%) of the patients had paroxysmal AF, amiodarone was not used in the control group and the study involved a small number of centers. Further study is therefore needed before ablation can be endorsed as first-line therapy for AF. … PV stenosis has a reported incidence of 1–38% Thromboembolic events due to catheter ablation of AF have a reported risk of 0–7%.. mitral valve damage secondary to trauma or catheter entrapment.” **While the ultimate value of these novel ablation technologies awaits the conclusion of a number of studies, there is optimism that electrophysiologists will soon have better tools for performing AF ablation, compared with the tools with which the field began.*** Advances in Afib 2009http://www.invasivecardiology.com/articles/Advances-Atrial-Fibrillation-Ablation **** Right Linear Ablation: Long Term follow Up Paroxysmal 1998: P, Shah DC, Takahashi A, et al. Long-term follow-up after right atrial radiofrequency catheter treatment of paroxysmal atrial fibrillation. Success rate: 53% after one year, 37% after two years. Long term attrition in success. (Pacing Clin Electrophysiol 1998;21:2533–2538)http://www3.interscience.wiley.com/cgi-bin/fulltext/119941498/PDFSTART A new system for catheter ablation of atrial fibrillation Hugh Calkins 1999 http://www.ajconline.org/article/S0002-9149%2898%2901034-0/abstract
FDA Trial Design 198 1A (Ablation for V Tac) PreMarket Approval for Chilli Catheter Brinker/Calkins… 30% major adverse event rate for Chilli Catheter. Journal article here: http://content.onlinejacc.org/cgi/content/full/35/7/1905#SEC2 Tracy: “I agree with the FDA reviewer that device labeling, page 218, the cooled tip ablation is referred to as a low risk procedure, and I think that is something that we are going to have to consider given that complications occurred in 44 out of 150 12 patients…” DR. SIMMONS: I would have thought that you had you know, 30 percent of the patients died, I mean there should have been some autopsy data, right? FDA Trial Design 1998 1C FDA Trial Design 1998 2A (Atrial Flutter – AFib starts p.99) FDA Trial Design 1998 2B (Afib ablation) Tracy: really pushing the technology we don’t know anything, p18/19 Just because you can, doesn’t mean you should” p16… I think that we are still so early in the learning curve with atria1 fibrillation, we don’t know anything about what lesions we really need, anything about what locations you need, whether they need to be transmural or not. We don’t know anything about it at all, so far, as far as I am concerned. P19 DR AZIZ hits it right on the head: doing patients like that. Basically, you are going to have a learning curve of people who are using the catheters. It may be that people who have been in A-fib for more than two years may not work out. I think it is a point where you are gathering data and if the patients are willing to take that chance– Page 116 FDA 1997 (Public Hearing File out and File back in) *** FDA clinical trial design transcript 2007 Part One FDA Clinical Trial Design 2007 Part Two FDA Clinical Trial Design 2007 Part Three FDA Clinical Trial Design 2007 Part Four FDA Clinical Design Trial 2007 Part Five FDA Clinical Design Trial 2007 Part six FDA Cardima Panel Pack P020039 Navistar Thermocool for JAMA study: FDA Summary of Safety and Effectiveness Data http://www.accessdata.fda.gov/cdrh_docs/pdf3/P030031S011b.pdf Navistar Thermocool Clinical Trial– Serious complication rate: Sixteen percent: http://www.accessdata.fda.gov/cdrh_docs/pdf3/P030031c.pdf Thermocool Clinical Trial Deflectable Tip — Serious complication rate: Eighteen percent: http://www.accessdata.fda.gov/cdrh_docs/pdf4/P040036c.pdfDR. WHARTON: I didn’t want to bring this up at this point but one of the issues that is going to have to made clear as you start designing protocols, and this came up actually with some of Dr. Haissaguerre’s work with rightsided linear lesions, but you have to define what you are doing. In Dr. Haissaguerre’s work, when they did a multivariate analysis of what predicted success from a right-sided-only procedure, it was who had a focal fib ablation which raises the issue that it wasn’t the rightsided lesioning at all. It was the focal-fib ablation that was the success. So, again, that is another issue in terms of outcomes and procedural methodology. At this juncture, though, I just want to make sure that FDA is clear that there are different types of fib ablation potentially that you are going to be presented protocols for, and they may not have the same protocol designs or the same type of inclusion criteria applicable, the two types, or three types. http://www.fda.gov/ohrms/dockets/ac/98/transcpt/3442t2b.pdf p46
Corruption/MISC
FDA Warns St. Jude for improperly marketing AF ablation devices (2010): http://www.cardiovascularbusiness.com/index.php?option=com_articles&view=article&id=22255&division=cvb Justice Department Charges Guidant:http://online.wsj.com/article/BT-CO-20100225-717543.html?mod=WSJ_latestheadlines Guidant Guilty Plea DOJ: http://www.justice.gov/civil/ocl/cases/Cases/Guidant/Plea%203-11-10.PDF $500,000 to Hopkins from Philip Morris: http://legacy.library.ucsf.edu/tid/ziw10c00/pdf;jsessionid=4035E6F05B21CF88E3B49C98B14EB3A6 Panel votes down proposal for non-RCTs for AF ablation use:http://www.accessmylibrary.com/article-1G1-169074616/panel-votes-down-proposal.html Off label use — http://www.eplabdigest.com/articles/Letter-Editor-%E2%80%9COff-label%E2%80%9D-Use-Ablation-Catheters-Atrial-Fibrillation Off label use: http://www.fredlaw.com/bios/attorneys/klepinskirobert/Klepinski_JMDRMay2009.pdf Atricure to Pay US $3.76 Million to Resolve Charges Medtronic defibrillator wires: http://online.wsj.com/article/SB10001424052748704259304575043300593884216.html?mod=WSJ_hps_LEFTWhatsNews Mergers and Aquistions Cardima p 69 http://dspace.mit.edu/bitstream/handle/1721.1/39576/174282482.pdf?sequence=1
http://www.massdevice.com/node/4270/20
Boston Scientific, Medtronic, five others slapped with off-label lawsuits
July 15, 2009 by MassDevice staff
Boston Scientific Corp.‘s notorious acquisition of Guidant Corp. is causing even more headaches for the Natick-based devices giant, now that a federal “qui tam” whistleblower lawsuit accuses the pair (and five other medical device makers including Medtronic Inc.) of promoting the off-label use of microwave cardiac ablation and potentially bilking millions from the Medicare system. The lawsuit accuses the two device giants, plus AtriCure Inc., St. Jude Medical Inc. and subsidiary Epicor Medical Inc. and Endoscopic Technologies of offering illegal kickbacks and free equipment to perform microwave cardiac ablation procedures not approved by the Food & Drug Administration. The suit alleges that Guidant (both before and after its April 2006 acquisition by BSC) initiated a scheme to encourage hospitals to improperly bill Medicare for the procedures and to “upcode” their bills to get even more out of the federal health program. The whistleblower, whose request that all personal information be redacted from court documents was granted, worked for Boston Scientific as a sales rep. According to court documents, she’s put in 16 years in the medical device industry and was a top 10 sales producer for a previous employer. During her training to sell Guidant’s Flex 10 ablation system, she was allegedly told to “market the spread” — that is, highlight the difference between what Medicare pays for cardiac ablations (an average $30,289) and the low cost of the Flex 10 procedure (an average $10,650). That $20,000 “spread” is pure profit for the hospitals. The scheme allegedly called for sales reps to coach hospitals to bill Medicare using codes for open-heart procedures, rather than the minimally invasive technique actually used, to bilk the system out of an extra $20,000 per procedure. The companies are also accused of providing free marketing and advertising to physicians in return for using the products, allegedly going so far as to pay for the design, printing and publication of brochures and ads. For hospitals or doctors who bought five of the devices, the companies would allegedly “loan” them microwave generators worth $28,000 and never ask to be repaid. And in return for locking in an agreement to use a company’s ablation system exclusively, sales reps were allegedly allowed to confiscate — or, in some cases, disable — competitors’ equipment in those hospitals. Cardiac ablation is a technique used to treat atrial fibrillation, or fast and irregular heartbeat. It’s a large pool of potential patients, as more than 2.2 million people have the condition and another 160,000 are diagnosed every year, according to court documents. Boston Scientific’s training materials allegedly estimated that U.S. hospitals stood to make $7 billion a year in Medicare reimbursements for treating atrial fibrillation. And the alleged marketing scheme was likely a windfall for the accused firms; Boston Scientific’s Flex 10 alone was used in 1,600 ablation procedures and in another 15,000 operations in conjunction with other procedures, according to the documents. At about $10,000 a whack, that adds up to $166 million in sales. When the whistleblower challenged the legality of the marketing scheme at training events and a national sales meeting, she was allegedly reprimanded and harassed before Boston Scientific fired her “as a direct cause of her acts challenging [Boston Scientific]’s marketing approach,” according to court documents. The lawsuit seeks triple damages and penalties of up to $11,000 for each violation. Under rules of the qui tam statute, which allows private citizens to sue on behalf of the government, whistleblowers are entitled to one-third of any damages and penalties won in a successful case. In addition to that, Jane Doe is seeking two times the amount of back pay and interest she would have earned if BSC hadn’t fired her, plus legal fees. San Ramon, Calif.-based Endoscopic Technologies agreed to pay $1.4 million to settle its part in the case. Federal investigators are still looking into the allegations against the other companies; the U.S. government has until August 21 to decide whether to join the qui tam cases against them. Trial Design 2007 2/pp140: ” …we sought input from a significant number of E.P.s. We were told by many of them that a study comparing A.F. ablation and medication did not make for strong clinical science because patients that failed a drug are being randomized to additional drug therapy as the control.”….. Burke Barett, vice president of regulatory and clinical affairs for CardioFocus. For the argument that too many patients fail drug therapy and that it is ineffective long-term, Prystowsky said that he has longitudinal follow-up on patients in his practice for an average of six years, with some patients managed on drug therapy for more than 10 years. Overall, more than two thirds of his patients have remained in sinus rhythm, he said, noting that this follow-up is three or four years longer than any existing ablation follow-up. – Prystowsky 2005 http://www.theheart.org/article/546039.do ic drug, the use of catheterablation compared with ADT resulted in a longer time to treatmentfailure during the 9-month follow-up period.” Brodsky: Calkins Meta Analysis Flawed: http://circep.ahajournals.org/cgi/content/extract/2/6/e44 When J&J had less heartening news to report, it didn’t do the full court press. This from a Reuters dispatch in 2005: Johnson & Johnson has revised the label of its Natrecor heart failure medicine to include data that suggest it may increase the risk of death, following two widely publicized medical journal articles that questioned its safety. J&J did not issue a press release to announce the label change. Instead, a company Web site, Sciosinc.com, published the lengthy label without pointing out which section of it had been added. “The label was quietly changed by Johnson & Johnson, which apparently doesn’t want to attract much attention to the new mortality language,” said Dr. Steven Nissen, a cardiologist at the Cleveland Clinic who in 2001 advised U.S. regulators not to approve Natrecor. *** Exec in Risperdal Kickback Case: “I Wasn’t Going to Jail for J&J” Jim Edwardshas been covering the writes in PharmaAnalysis According to data appearing today in JAMA, patients with a common heart rhythm disorder, called Atrial Fibrillation, who were treated with catheter ablation using the NAVISTAR® THERMOCOOL® Catheter, demonstrated significantly better outcomes at one year compared to those receiving drug therapy. In addition, the patients treated with catheter ablation reported markedly fewer symptoms and substantially improved quality of life. http://news.moneycentral.msn.com/ticker/article.aspx?Feed=BW&Date=20100126&ID=11060705&Symbol=JNJ **** In 2007, with his patient recruitment piece still up on the Hopkins site, he wrote an opinion piece for the journal Nature in 2007, in which he recommended that catheter ablation for Afib should not be considered as a first line therapy. He begins by repeating what he told the FDA four years earlier, that “The true efficacy of Afib ablation remains unknown.” **** There is no question that Hopkins is fighting this lawsuit not about money, they have already spent enough to demonstrate that. It’s about about their business model, which requires a burnished reputation by which to gain the confidence of those searching for medical help. The trainees get paid by device manufacturers. Hopkins contends that the term traineecarries a negative connotation, and points out that these are full Medical Doctors on fellowships. The Fellowships are paid for by medical device manufacturers. Richard Wu, for example, might have been the BioSense Webster Fellow at Hopkins in 2002. When Barbara Bean sent Pam’s records to her new cardiologist, she included this note: “She has a lawsuit pending against Johns Hopkins.”
BioSense Webster Lasso Catheter Recalled
http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfres/res.cfm?id=69666Recall Number: Z-1703-2008 and Z-1704-2008. See FDA weekly enforcement report for more details about the recall. This recall was initiated on March 25, 2008 by Biosense Webster for the Lasso 2515 Variable Circular Mapping Catheter, US Catalog Number D7L202515RT. This recall was initiated after the firm received several complaints reporting issues with deflection. The catheter may become caught in the mitral valve, requiring surgical procedures, valve may be torn while trying to dislodge, unable to retract the catheter through the sheath and require surgical intervention to remove, pulling on catheter to remove may lead to large atrial septal tear, and separation of the distal end of the catheter may occur. Also, the firm determined that when the catheter is fully deflected and the variable loop is fully contracted, it is possible that the catheter mechanism can become “locked” in position and cannot return to the un-contracted, un-deflected state. This could lead to damage to the device or limit the ability to withdraw the catheter safely. Call Diana M. Thorson 909-839-8604
A History of GI Bleeding
Mallory Weiss
Richard Wu
So that’s why he was all shaken up when he stood next to Hugh Calkins that afternoon in 2002. By the time we found that out, litigation was under way. I thought, I’ll just get hold of Dr. Wu and have him write a statement about how he had never met my wife. This would prove that Hugh Calkins had tricked and misled us. Wu was working at the University of Texas Southwest Medical Texans like their heart centers and it is a big deal to be the Dallas Heart Ball Chair in Cardiac Arrhythmia Research at The University Texas Southwestern Medical Center. 
America’s Best Hospital
The experience begins when you drive up to the front of the hospital, a large and impressive structure built on a hill. There is a professional valet staff; crisp, cordial and efficient like at a swanky hotel. The doors slide open as you walk into a large atrium. Before you have a chance to feel lost, you are met by a smiling greeter who sorts you and sets you on the right path. Before you know it, you have surrendered your autonomy and are sitting in a wheel chair while a uniformed staffer is pushing you down a long corridor paneled on both sides with posters of Johns Hopkins Medicine on the cover of US News and World Report. You have put your life into the hands of the institution.
” She was a Nurse”
DR. MORRISON: Well, I would just like to ask the other members of the panel if any of them are as shocked as I am to hear the FDA say we’re designing trials where the sample size is based on safety rather than efficacy. ****** Sanjeev Saksena, M.D. (Look up) “… the first survey, worldwide survey, on atrial fibrillation demonstrated that percent of the patients who were deemed effectively treated with atrial — for atrial fibrillation by ablation had that success associated with the need for anti-arrhythmic drug therapy. The protocol is designed so that if a retreatment is within two months, it’s considered not a treatment failure. And yet clinical practice is typically to delay retreatments beyond two months because we all know about delayed healing, and there’s certainly an inflammatory phase that can go on for three months or longer. So this, obviously, is a difference between how the study was designed and what is considered best clinical practice to date.” Calkins FDA2007#2p27 ” … we all know that once you’ve failed your first anti-arrhythmic drug, that almost guarantees you you’re going to fail your second or third anti-arrhythmic drug. So the current way drugs are mandated, I think, is very cumbersome. “And I think the entire field would benefit tremendously from saying if you failed a beta blocker or calcium blocker, you could be randomized to ablation or an anti-arrhythmic agent, and that would give you a more effective comparator and, I think, help enrollment a great deal in all of these trials.” Calkins FDA 2007#2 p 29 As a practicing electrophysiologist who does these procedures, I’m very eager to have objective evidence demonstrating particularly the safety and efficacy. Dr. Slotwiner DAF 2007 # 2 page 60 *** Dr. David Eddy proved again and again that the emperor had no clothes. “The intellectual foundation of medical care is based on the assumption that whatever a physician decides is, by definition, correct. While many decisions are, no doubt, correct, many are not, and elaborate mechanisms are needed to determine which are which.” **** Hugh Calkins could not have explained the risks and benefits of catheter ablation for atrial fibrillation to Pam because he did not know what the risks and benefits were. In fact, performing the procedure on Pam was how he was hoping to find out what the risk/benefit ratio was.
****
Lawsuit Challenges Marketing of Stents
By BARRY MEIER
A former medical device executive claimed in a potential whistle-blower lawsuit that was unsealed this week that the makers of stents approved to treat digestive tract cancers had illegally marketed them for years to treat blocked blood vessels in other parts of the body. In the lawsuit, Kevin N. Colquitt, a former regional sales director for Guidant, stated that he had been trained to market the devices, which are known as biliary stents, to doctors for off-label uses not approved by the Food and Drug Administration. **** ***** “We commonly saw what looks like a gunshot blast where you have one lesion here, one lesion here, one lesion here, one lesion here, nothing continuous or linear about it. Whether these lesions are in fact pro-rhythmic, anti-arrhythmic, who really knows… (emphasis added) this new catheter would be more doing what we are trying to do which is not ablate the atrium but put road blocks up to ablate atrial fibrillation.” So it appears that at least one interventional cardiologist performing the procedure was fully aware of “the level of destruction created in a patient’s left atria.” In 2003, Hugh Calkins was trying to sell the FDA on Cardima’s new catheter on the grounds that it would help cardiologists not obliterate the inside of the left atrium. Imprecise, blundering obliteration may have been what he was practicing, but it’s not what he was selling. It’s not the picture he presented for public consumption. It’s not what the David Erdmans of the world were told – because, how else would you learn? One has to wonder about the motivation for the duality in Calkins’ portrayals of the procedure to his different audiences. Two of his public pronouncements in 2006 illustrate the contrast between selling to perspective research subjects (patients) and reporting to colleagues. In “The Arrival of A-FIB Ablation” on the Hopkins website, the good news is delivered to AFIB suffers that their worries are practically over: Dr. Calkins “delivers radiofrequency energy around the outside of the pulmonary vessels to knock out the source of the aberrant electrical signal. A-fib episodes may still occur for a few weeks, but most patients are free of them within a month.” Free at last! Thanks Doc! But he has more sobering news for fellow researchers in a Cardiosource journal article that came out at the same time: “Hugh Calkins, MD, FACC, recently co-authored a worldwide survey on the methods, efficacy, and safety of catheter ablation procedures for AF… (Only) 52.0% of catheter ablations proved “curative”… Also, it should be noted, 24.3% of patients required a second ablation procedure… The overall incidence of major complications was 6.0%, which the authors noted “is not trivial.” Complications included …death, tamponade, aortic dissection, stroke, and PV stenosis. Further, Calkins says, “We really do not have a true handle on the long-term efficacy of this procedure. Also, I personally have a problem with physicians who make the statement that their patient’s atrial fibrillation is cured by catheter ablation. We really don’t have data to support that claim.” In another illustration of the difference in the two faces put on the procedure is that generally, when Hugh Calkins talks about having to repeat the entire process because it failed the first time, he’ll tell his peers that the patient needs a second procedure, a third procedure. When Hugh Calkins talks to prospective patients, uses the phrase “touch-up.” Why does he do this? In 2007, with his patient recruitment piece still up on the Hopkins site, he wrote an opinion piece for the journal Nature in 2007, in which he recommended that catheter ablation for Afib should not be considered as a first line therapy. He begins by repeating what he told the FDA four years earlier, that “The true efficacy of Afib ablation remains unknown.” I don’t know about the rest of the hundreds, perhaps thousands of other patients that Hugh Calkins “steered toward” what he called “the most dangerous procedure that electrophysiologists do,” but he most definitely did not tell Pam and me that he had no idea whether the procedure actually worked. (I would have distinctly remembered if a doctor recommended a procedure, told me that it would be the most risky and dangerous thing he ever did, that the complication rate is unprecedentedly high — and then said that he didn’t even know if it worked.) Calkins goes on to say that “serious complications continue to occur even in the most experienced hands… New, devastating complications are emerging. Perhaps the most frightening of these is esophageal perforation, which is often lethal — and atrioesophageal fistulas, which are perhaps the most feared and most lethal of the many complications that have been associated with this procedure – with mortality in excess of 75 percent… and new complications are being ‘discovered’ on a regular basis…” “Some doctors are pretty enthusiastic about ablation as a primary therapy,” Calkins says, “but they’re only enthusiastic until a patient has a stroke or some type of devastating consequence. Then the enthusiasm tends to go down a little bit.” Ah, the learning curve. **** hopefully by then we’ll know what tools are the best to do it with and we’ll have a little more information so we can do it more safely.” **** ****** The Heart.org: Is more conflict of interest disclosure getting us closer to the truth? http://www.theheart.org/article/963203.do ****** BusinessWeek Medical Guesswork: http://www.businessweek.com/magazine/content/06_22/b3986001.htm Calkins “So anyhow I went ahead and started doing the procedure and these are the results we saw in our first 75 patients….” [ In addition to the destruction of my wife’s heart valve, the procedure caused three people to have holes poked in their hearts, three other people to have strokes, and six people developed pulmonary vein stenosis. Out of 75 people who underwent the procedure, 11 people had it done twice. Twenty six people experienced no benefit whatsoever. The 39 people for whom the procedure was counted as successful were only followed for eights months, and it was becoming clear that Afib returned more and more often as time went by.] The longer you follow the patient, the more Afib recurs. . for persistent or permanent Afib this procedure is just awful – a 20% success rate. Complications, they were memorable two strokes, [not counting Pam’s] three tamponades, the mitral valve Lassoed, Pulmonary Vein stenosis, some vascular complications. … this was not the answer, at least for the patients that I had to deal with and deal with the aftermath. Circumferential ablation (worked a lot better, very impressive, breeze through the complications, Let’s take a harsh look at our numbers and see how we really did, and it was somewhat appalling, I think our success rate was about 35% — our success rate for single procedure outcomes with 12-moth follow up — with a 7% complication rate. And my colleague Ron Berger says, you can’t publish these data, we’ll never see another patient again at Hopkins. Can you find a silver lining? So we did identify a subset of patients with paroxysmal afib that were young that had small left atrium that had blue eyes that had a 70% success rate, but for the rest, the success rate was much worse… **** Jeff Brinker was called at xxxpm, arrived at 2xx pm yanked on the catheter at # pm. What had he been doing when Calkins called. Was he in the middle of training the other fellow? Wu says he discussed alternatives like drug therapy and doing nothing. Calkins had already falsely declared that Pam had failed three anti-arrhythmic drugs. Why would Yuh be offering her the option? ****************** “Staffing for ablations should consist of at least three team members in addition to the attending physician. It is “recommended that staff utilized for ablative procedures have experience with at least 30 catheter ablations before working independently in the EP lab, and that they continue to assist on 30 cases per year.” – Hugh Calkins, NASPE Policy Statement on catheter ablation: Personnel, policy, procedures, and therapeutic recommendations. PACE 2003;26:789–799
|
|
| Reply To This Message |
| Re: Andrea Natale Appointment | |
|
|
| Reply To This Message |
| Re: Andrea Natale Appointment | |
|
|
| Reply To This Message |
| Re: Andrea Natale Appointment | |
|
It is likely that Richard Wu’s salary was being paid by a medical device manufacturer… http://www.mddtransparency.com/sites/default/files/file/Biosense_Webster/BWI_%20Q109Grants%20090617.pdf Boisense Webster Largess to Johns Hopkins… EP Fellowship Program ‐Jan‐ 09 JOHNS HOPKINS UNIVERSITY BaltimoreMD $50,000.00 **** ***** Ten days before Pam and I pulled up to valet parking at Hopkins for the big event, officials from the organization were down in the state capital fighting like hell against a bill that would tighten oversight of research studies with human beings as subjects. Medical research bill opposed at hearing Biotech industry, universities against adding state oversight By Tom Pelton, The Baltimore Sun (Sun Staff) Originally published March 15, 2002 http://www.circare.org/media/31502BS.pdf *** FDA Warning Letter Hints at Crackdown on Unregulated Research, IND Enforcement By M. Alexander Otto BNA’s Medical Research Law & Policy Report May 7, 2003 A recent letter from the Food and Drug Administration to Johns Hopkins University in Baltimore contains what may prove to be the start of agency efforts to bring unregulated human experimentation under federal oversight, according to BNA interviews with key FDA personnel http://www.circare.org/bna05072003.pdf ***** “The process of atrial fibrillation ablation is really exploding out there regardless of whether it’s approved, simply because it works,” Hugh Calkins, M.D., of John Hopkins, an electrophysiologist who consults for Johnson & Johnson, told the advisers. Working for J&J Navistar ’08 http://www.medpagetoday.com/ProductAlert/DevicesandVaccines/11880 *************** ********** January 29, 1997: 510K for Pathfinder RECORDING catheter: http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMN/PMNSimpleSearch.cfm?db=PMN&ID=K955802 In a 1999 SEC filing Cardima writes that “Although our microcatheter products are labeled for single use only, we are aware that some physicians are reusing such products. Moreover, despite labeling of our microcatheters for diagnostic use only, we believe that physicians are using such mapping microcatheters for ablation.” What would lead Cardima to believe that physicians were using mapping catheters to perform ablations, which is contrary to their approved use? It might have been this press release they sent out the year before: Cardima Successfully Treats First Patient in United States Atrial Fibrillation Study at the Johns Hopkins Hospital FREMONT, Calif.–(BW HealthWire)–April 3, 1998– [K971975 July 1998] Cardima, Inc. today announced that the first patient in its (AF) ablation feasibility study was successfully treated last week. The patient, a 38 year old male who had been suffering from almost daily episodes of AF for over five years, was treated and left the hospital in normal heart rhythm. Ronald D. Berger, M.D., Ph.D., a cardiac electrophysiologist at the Johns Hopkins Hospital, treated the patient using the Cardima Pathfinder ablation catheter. Dr. Berger said, “This was a highly symptomatic man who had been suffering from AF with no potential for a cure available in the near future. We were delighted to enroll him in Cardima’s clinical trial and treat his AF in a minimally invasive fashion. We had considered a highly invasive open heart operation called the maze procedure on this patient, but felt the minimally invasive approach would be safer in this instance. Cardima’s product offered the option of a catheter-based maze procedure and we are extremely pleased with the results.” Dr. Berger cautioned that long-term follow-up will be required to further assess the success of the procedure… Phillip C. Radlick, Ph.D., President and Chief Executive Officer of Cardima said, “We are pleased with the outcome of this very difficult case. It is gratifying to see a successful patient outcome, especially for a person who had suffered for as long as this gentleman did. Approximately four million people in the world suffer from this condition, with no cure currently available. We will strive to complete the U.S. ablation feasibility phase of our trial … Additionally, our European clinical trial for treating AF through ablation is proceeding on track. We have treated 12 patients to date in this trial,all of whom were in normal heart rhythm after the procedure. [Of course they were: all patients are discharged from the hospital on amiodarone or similar drug] At the completion of the trial, we will submit the data in our application for a CE mark which will permit us to market the product in the European Union.”
Email from the FDA:
“The cardiac device, The Pathfinder, was cleared for marketing by the Food and Drug Administration (FDA) in 1998: The developer is Cardima, Inc. You should know, though, one of the FDA’s device experts tells us, the intended use of the device seems to be different from what you are asking about in your e-mail. You may want to check clinicaltrials.gov to see if there are any new studies in this area.
Very Respectfully,Eugene J. Koprowski and Nancy Bruening”
Cardima 10Q June 1998 Although the Company has received regulatory clearance to market the Cardima Pathfinder and Pathfinder Mini microcatheter systems for mapping VT and the Revelation microcatheter system for mapping AF, none of the products currently being developed by Cardima for ablation of AF and VT has received regulatory approval in the United States.
Journey to the Far Side:http://www.secinfo.com/dut49.72zh.htm#aug
Currently, there is considerable clinical debate about the needfor mapping AF prior to ablation, and no mapping is performed during the openheart surgical maze procedure. However, the Company believes that mapping priorto ablation may be useful to identify different segments of the AF population,each of which could require slightly different mapping and ablation procedures.For example, some electrophysiologists believe most AF patients will need to bemapped and ablated in both the left and right atria, while others believe onlythe right atrial intervention is warranted. Market acceptance of this productfor mapping will depend largely on a determination that there is a clinical needfor diagnostic mapping prior to ablation of AF. The Revelation Tx ablationprocedure may require the use of RF energy in both the right and left atria toproduce lesions. In general, the use of RF energy in the left atrium has thepotential to create blood clots, which could travel through the vasculature tothe brain and may cause a stroke...
http://tinyurl.com/Nightmaresin-AFibAblation
"The FDA's prohibitions against promoting approved products forunapproved ("off-label") uses."
Cardima :BIG MONEY 1997 Pathfinder Berger”The company has been funded by a variety of venture capital firms, including Kleiner, Perkins, Caulfield and Byers; Goldman Sachs; Chase Venture Partners; New Enterprise Associates; Premier Health Ventures; and Atlas Ventures.http://findarticles.com/p/articles/mi_m3570/is_n10_v20/ai_20043173/pg_2/?tag=content;col1 FREMONT, Calif., Oct. 6 2000 /PRNewswire/ –Cardima, Inc., (Nasdaq: CRDM) announced today it has treated the first patient in Phase III of its atrial fibrillation (AF) clinical trial. Dr. Hugh Calkins of the Johns Hopkins Hospital treated the patient. “The patient was a 68 year old female with a 10 year history of paroxysmal AF,” stated Dr. Calkins. “We treated her with the Revelation Tx and Cardima’s new NavAblator catheters, the patient tolerated the procedure well and she has returned to work. The evaluation of this new therapy is ongoing. I am very pleased with the outcome of this case and the performance of Cardima’s products.” “We are very pleased to treat the first patient in Phase III of the clinical trial,” said Gabriel Vegh, President and Chief Executive Officer of Cardima. “We continue to focus our development efforts on therapies that significantly reduce or eliminate AF as opposed to supportive therapies with devices such as pacemakers.” **************** the technology is way ahead of the science. That’s always a problem. I think that’s where we are now and we have made advances in this field.- Dr. Waldo ******** American Heart Association’s Annual Scientific Sessions, Dallas Dec.2001 He first did a 10-patient feasibility study, then a Phase II trial, and finally a pivotal trial, currently in progress. Calkins said that the results of the first 48 patients can be interpreted based on “what type of person you are — an optimist or a pessimist. If you’re a pessimist, you’d probably say, `47 out of 48 patients had atrial fibrillation again, and it doesn’t work.’ But if you’re an optimist, you’d say, `my goodness, look at this tremendous reduction in afib burden.'” He cited the example of a patient with more than 50 AF episodes a month, now down to just four per month. Additionally, data from six-month follow-up demonstrated more than a 100% reduction of episodes in half the patients and a 50% reduction in episodes in 87% of the patients. The real issue here, he said, is quality of life, “since afib doesn’t kill you.” Calkins said that he personally called some of the patients who had participated in the trial from one to three years previously, and asked about their condition. A total of 21 patients responded and said they were now minimally symptomatic. Summarizing these preliminary results, he told his breakfast audience that radiation ablation using the Cardima system “demonstrates that it’s safe, it seems to reduce the afib burden results in long-term elimination of afib in up to half the patients and improves [their] quality of life.” Calkins Scientific Sessions, Dallas Dec.2001 http://www.accessmylibrary.com/coms2/summary_0286-27267181_ITM ********************* “It is not advisable to draw conclusion from these data…” FDA statistician on PMA20039. Equipment failures during trials pg 96 PMA20039… IN March, 2002, a Press Release went out announcing the big date for the presentation. http://www.medscape.com/pages/editorial/pressreleases/pr-crm-cardima1 ************************** Business Wire May 14, 2003: Dr Calkins will discuss linear ablation as a less-invasive alternative to the MAZE procedure. Smithsonian Cardima to Host Scientific Symposium at NASPE Thursday, May 15, 2003 ****************** January 7, 2003 • Cardima (Fremont, California), developer of the Revelation Tx and Helix microcatheter systems for treating atrial fibrillation (AF), has completed a private placement of 4.36 million shares of common stock to select accredited investors at a price of about 75 cents per share. The private placement also included the issuance of warrants to purchase up to an aggregate of about 2.4 million additional shares of common stock at an exercise price of approximately 82 cents per share. Net proceeds to the company were about $3 million. http://www.medicaldevicedaily.com/img/mdd_sample.pdf Calkins for Cardima at the Smithsonian: http://findarticles.com/p/articles/mi_m0EIN/is_2003_May_14/ai_101684079/ The article includes comments by Dr. Hugh Calkins, professor of medicine and Director of Electrophysiology Services at Johns Hopkins University, in Baltimore, who participated in the right-sided linear ablation trial for the Revelation Tx. According to Dr. Calkins, “Three months after ablation 38% of patients had no AF and six months after ablation 47% had no AF.” Additionally, Dr. Calkins noted that the study group had significant episode reduction in symptomatic AF. The study group recorded an average of 10 AF episodes per month prior to ablation, an average of 3.7 AF episodes per month three months after ablation, and an average of 1.9 AF episodes per month six months after ablation. Dr. Calkins commented, “This is the first prospective, multi-center clinical trial for catheter ablation of atrial fibrillation that has reached the finish line. I think that’s the enormous hurdle that has been crossed. There were about 10 other companies that started the race, but all the rest packed it in. Cardima had the fortitude to stick with it and present us with results.” Dr. Calkins further noted that catheter ablation resulted in a significant improvement in quality of life. “I think catheter ablation will be routinely performed to cure afib — that’s clearly where we’re moving,” he commented. Cardima, Inc. developed the REVELATION(R) Tx linear ablation microcatheter system as a minimally invasive, single-use product that may have the potential for curing AF. The REVELATION(R) Tx linear ablation microcatheter system is believed by the Company to be the first device to treat AF that has completed a multi-center clinical trial and has had a pre-market approval (PMA) application submitted to the FDA. Cardima submitted the PMA on September 20, 2002 and was granted expedited review status by the FDA on November 5, 2002. Clinical trial data from the REVELATION(R) Tx microcatheter demonstrated safety and promising efficacy. Cardima’s mission is to get better devices to treat AF in the hands of the medical community. ************************* “The panel members noted that Cardima’s primary investigators “contaminated the data” The panel noted this clinical trial was not a prospectively defined trial from the onset, and that the primary investigators “did not play by the rules that they designed, and furthermore, should have been eliminated from the clinical trial as primary investigators” (Dr. White). The panel also noted that missing data from the clinical trial did not translate to mean that patients did not experience episodes. Therefore, there was a lack of rigor and robust data (per Dr. Waldo, Dr. White, and Dr. Norman). In addition, the panel members concurred with the Agency’s recommendation that the increase of amiodarone dosage would be considered a clinical failure. Most importantly, the panel noted in thclr final remarks that this was an “observational exercise” and not a true clinical trial. Since the data was improperly collected, there was no way to salvage any information from this study. It is the Agency’s understanding that the sponsor would hare to start again at the Pre-IDE level. Finally, the panel found very little evidence to support reasonable assurance of safety and effectiveness for the Cardma catheters (the Revelation TX and the Navablator)….Finally, the panel found very little evidence to support reasonable assurance of safety and effectiveness for the Cardima catheters… ********* ******* http://tinyurl.com/Cardiac-Pathways (Leveraging electrophysiologists) FOIA Food and Drug Administration Freedom of Information Staff (FOI) 5600 Fishers Lane , HFI-35 Rockville , MD 20851 (301) 827-6500 (voice), (301) 443-1726 (fax) **** Cardima:Medical Device Daily Features Cardima’s Technology to Treat Atrial Fibrillation. Cardima: http://www.medscape.com/pages/editorial/pressreleases/pr-crm-cardima1 http://tinyurl.com/EthicalIssuesCardiology ********** CALKINS: Among these sources of outcome data, it is well recognized that data derived from large prospective randomized clinical trials most accurately reflect the outcomes that can be anticipated when a procedure is performed in clinical practice. Unfortunately, as of the time this document was prepared, there have been no large randomized multicenter clinical trials performed to determine the safety and efficacy of catheter ablation of AF. http://www.medscape.com/viewarticle/558137_3 2007 ***** CALKINS Mitral valve trauma Entrapment of the mitral valve apparatus by a curvi-linear electrode mapping catheter is an uncommon complication of AF ablation.290Go,291Go It results from inadvertent positioning of the circular electrode catheter into the ventricle with counterclockwise rotation of the catheter resulting in entrapment of the circular catheter in the mitral vale apparatus. When suspected, it is important to confirm the diagnosis with echocardiography. Although successful freeing of the catheter has been reported with gentle catheter manipulation and advancing the sheath into the ventricle, great caution must be used as it is possible to tear the mitral valve apparatus. It is recommended that if gentle attempts to free the catheter fail, elective surgical removal of the catheter should be performed. http://europace.oxfordjournals.org/cgi/content/full/9/6/335?ck=nck#EUM120C51 (2007) Cardima submitted the PMA to the FDA on Sept. 20, 2002, and was granted expedited review status by the FDA on Nov. 5, 2002. Cardima announced on March 6, 2003, that the FDA has set a May 29, 2003, Circulatory System Devices Panel date to review the REVELATION(R) Tx PMA application. Clinical trial data from the REVELATION(R) Tx microcatheter demonstrated safety and promising efficacy. http://www.allbusiness.com/legal/health-care-law-drug-medical-devices-approval-fdas/5716900-1.html
****
§4–401 of the Maryland Code
A provider may not knowingly or willfully destroy, damage, alter, obliterate, or otherwise obscure a medical record, hospital report, laboratory report, X-ray report, or other information about a patient in an effort to conceal the information from use as evidence in an administrative, civil, or criminal proceeding. A provider who violates any provision of this section is guilty of a misdemeanor and on conviction is subject to a fine not exceeding $5,000 or imprisonment not exceeding 1 year or both.http://mlis.state.md.us/asp/web_statutes.asp?ghg&4-401
Clyde W. Yancy, MD, FACC, FAHA
Disclosure: Clyde W. Yancy, MD, Professor of Medicine/Cardiology, University of Texas Southwestern Medical Center, Dallas; Director, Heart Failure/Heart Transplantation, St. Paul University Hospital, Dallas, Texas has disclosed that he has received grants and clinical research support from GlaxoSmithKline, Scios, Medtronic, and NitroMed. Dr. Yancy has also disclosed that he has served as a consultant for GlaxoSmithKline, AstraZeneca, Scios, Medtronic, and NitroMed. Dr. Yancy has also disclosed that he has served on the speaker’s bureau for GlaxoSmithKline and Novartis
ACC/AHA/ESC Guidelines for the Management of Patients With Atrial Fibrillation 2001: http://circ.ahajournals.org/cgi/content/full/104/17/2118“Ablation of these foci eliminates or reducesthe frequency of recurrent AF in more than 60% of patients,but the risk of recurrent AF after a focal ablation procedureis still 30% to 50% over the first year and even higher whenmore than 1 pulmonary vein is involved. Thus, many patientscontinue to require antiarrhythmic drug therapy after ablativetherapy of AF (153). Potential complications of catheter ablationfor AF include systemic embolism, pulmonary vein stenosis, pericardialeffusion, cardiac tamponade, and phrenic nerve paralysis. Thus,although these procedures have produced promising results, theyhave not yet been widely applied.” Circulation November 7, 2000 “Dofetilide should be considered an important new treatment option for patients with AF”” The treatment should not be worse than the disease itself.”http://circ.ahajournals.org/cgi/reprint/102/19/2385?ijkey=1afa008ccb8bbf6da31ae357458ca7e37315ae91 Wellens HJ. Pulmonary vein ablation in atrial fibrillation: hype or hope? Circulation. . 2000; 102: 2562–4. http://circ.ahajournals.org/cgi/ijlink?linkType=FULL&journalCode=circulationaha&resid=102/21/2562Dofetilide is “Proven Effective for Pharmacological Cardioversion of Atrial Fibrillation.”
“Uh… You Weren’t There that Day…”
I couldn’t believe what I was hearing. I was listening on an old Bakelight telephone I’d picked up at the Goodwill years before. It sounds much more clear than any telephone manufactured today. So when Hugh Calkins told me an out and out lie, there was no mistake about it. After months and months of research, trying to understand what went wrong, it dawned on me one evening that we were not told how risky catheter ablation for atrial fibrillation was. I had been reading medical journals Agency’s Freedom of Information Office, Room 12A-15 of the Parklawn Building ***** in2001: The concept of catheter ablation of focal atrial fibrillation emerging as a first line treatment option is likely to become a reality. in 2006: catheter ablation of AF in general should not be considered as first line`therapy. It is important to recognize that catheter ablation of AF is a demanding technical procedure that may result in complications. Patients should only undergo AF ablation after carefully weighing the risks and benefits of the procedure…. http://www.hrsonline.org/Policy/ClinicalGuidelines/upload/HR-and-Euro-Copy-for-Print.pdf
The Internet
1999 Bad year for Cardiac Pathways. Sunnyvale’s Cardiac Pathways Corp., a maker of heart diagnostic products, was at the very bottom of the list, with its stock down 82 percent for the year. The company is still awaiting approval from the U.S. Food and Drug Administration for a system that uses ultrasound technology to treat heart abnormalities. (Year End 1999) http://www.sfgate.com/c/a/2000/01/01/BU106661.DTL Top U.S., European Physicians Discuss Clinical Application at Pre-NASPE Symposium WASHINGTON–(BW HealthWire)–May 17, 2000 The RPM system, the only commercially available system to integrate real-time, 3D-catheternavigation with state-of-the-art ablation technology, is designed to assist physicians in accurately manipulating catheters within the heart during procedures without the aid of fluoroscopy examination by means of the fluoroscope. The Chilli Cooled Ablation System uses closed-path fluid circulation to control the catheter tip temperature during ablation. By controlling the temperature, electrophysiologists are better able to deliver energy to ablate cardiac tissue responsible for the arrhythmia arrhythmia , disturbance in the rate or rhythm of the heartbeat. Various arrhythmias can be symptoms of serious heart disorders; however, they are usually of no medical significance except in the presence of . Design improvements to the Chilli catheters enable clinicians bi-directional steering capability in real-time and integrate the company’s ultrasound transducer transducer, device that accepts an input of energy in one form and produces an output of energy in some other form, with a known, fixed relationship between the input and output. technology. “Used together, these new, groundbreaking products provide electrophysiologists with the toolsand the technology that will deliver improved productivity for the EP lab. It is our hope toprovide a better quality of life for patients with arrhythmias by using a procedure that is safe,easy to use and cost-effective,” said Thomas M. Prescott, President and CEO of Cardiac Pathways. Hugh Calkins, M.D., an electrophysiologist with John Hopkins University of Medicine and PublicHealth, spoke to the system’s utility during a pre-NASPE symposium at the Grand Hyatt Hotel lastnight. Dr. Calkins, along with his colleague, Dr. Ronald Berger, has performed a number of procedures using the Cardiac Pathways’ RPM system and has been impressed by its ease of use and intuitive nature. “The 3D display of information enables the creation of linear lesions to within 1-2 millimeters of accuracy,” Dr. Calkins said. “I can see the entire scope and trajectory of the catheters, and it is my hope that I will be able to manipulate the catheters within the system, so I will no longer need to use fluoroscopy.” *** Wharton 2001 It is clear from the available information that curative ablation approaches for AF are rapidly advancing, but too little is known at present to advocate widespread implementation. In particular, given the potential for serious complications, even with ablation of AF initiators in healthy individuals, it is difficult to advocate ablation as front line therapy in advance of traditional pharmacologic approaches. Furthermore, the procedures are technically difficult, arduous, time-consuming, and are not cost-effective. Given the risks of serious complications, even in experienced hands, a loud note of caution must be expressed concerning widespread application by individuals who are inexperienced in technical aspects of the procedure, such as trans-septal catheterization, pulmonary vein ablation, and linear lesion creation in the left atrium. Appropriate educational guidelines need to be established in order to ensure safe application of these approaches in the community….More importantly, rates of major complications in the prospective studies have been unacceptably high, occurring in approximately one-quarter of patients. Although symptomatic control with continued antiarrhythmic drug therapy can be achieved in the majority of patients, the high rates of serious complications significantly limit application of these procedures to only a few, heavily symptomatic patients, and hamper enrollment of patients in studies evaluating new technologies that are aimed at simplifying the procedure. Limitation of the linear lesions to the right atrium greatly simplifies the procedure and avoids the potential risks associated with creation of linear lesions in the left atrium. Right-atrium-only linear lesion sets rarely cure patients with paroxysmal AF, however, and are ineffective in chronic AF [16,19,20]. Selected patients with paroxysmal AF may have high rates of cure [20], but the criteria for selection of these patients are not well defined. http://tinyurl.com/Wharton2001 Calkins Linear lesions, 2007: However, this strategy may be counter-productive, as linear lesions may themselves be proarrhythmic, especially if incomplete. CALKINS 2007 “… Over the past five years, the technique of catheter ablation for atrial fibrillation (AF) has evolved from being an experimental procedure…” http://www.medscape.com/viewarticle/558370_4 Calkins 2007: Entrapment of a catheter in the mitral valve results from inadvertant positioning of the catheter into the ventricle with counterclockwise rotation… Heart Rythym, Vol. 4 No. 6, June, 2007 http://www.i-sis.org.uk/isisnews/i-sisnews11-14.php: #### Scientists at Johns Hopkins serve as paid consultants and scientific advisers to corporations. The university filed more patent applications in 1999 than all but two other major research centres. It helped launch 18 companies in recent years, and corporate-sponsored research at the medical school has nearly quadrupled in the past decade. Johns Hopkins is taking a permissive attitude towards its scientists researching products on which they have financial stakes. For example, a senior scientist was allowed to test an experimental vaccine developed by a company he co-founded. Tiny Magnetic Resonance Imaging devices were tested on humans by scientists who invented the devices, developed by a company that the scientists and Johns Hopkins partly own. Dr. Bart Chernow, then vice dean of research at the medical school, proposed a business partnership to Craig Venter of Celera, the private company that sequenced the human genome, back in 1998. He boasted that Johns Hopkins was “one of the biggest biotech companies in the world”, and suggested that the school could supply Venter with blood and tissue samples from some of the 100,000 patients that Johns Hopkins scientists see each year. “There is this supposed immorality in trying to patent genes and develop new medicines,” Chernow said, shaking his head. But Johns Hopkins, he said, had finally recognised that industry was not its adversary but its greatest ally. On 19 July 2001, the US government ordered a suspension of all clinical trials in Johns Hopkins following the death of a previously healthy 24 year old volunteer in an asthma experiment, for which the University accepted full responsibility. The shutdown lasted 3 days, but 2 200 research protocols will have to be reviewed by ethics board before they can recommence [6]. ______________________________________________________________________________________________ http://www.hindu.com/fline/fl1817/18170090.htm The most striking example for well-known academic-research institutions in the U.S. having such links with industry is perhaps the Johns Hopkins University (JHU) itself. Spurred by the fear of being left behind in the race for research funds and top-notch faculty and students, the institution, once dedicated to pure research, is now in the forefront of universities trying to forge partnerships with business. After the cancellation of federal funds following the death of a “healthy volunteer” participating in an asthma study at the JHU on June 2, the university has remained in media focus with regard to the growing involvement of clinical investigators and research institutions with business. According to a report in The Baltimore Sun, the university had filed more patent applications in 1999 than all but two other major research centres in the U.S. Moreover, in recent years the JHU had helped launch 18 companies, and the volume of corporate-sponsored research at its medical school had nearly quadrupled in the last 10 years, the report said. http://www.cardiosource.com/ExpertOpinions/hottopics/article.asp?paperID=228 ________________________ CALKINS: “I think all of us are aware of the fact that the published literature probably tremendously overestimates the true efficacy of catheter ablation…”http://tinyurl.com/CalkinsFDAProRhythm 2007 DR. YANCY: This is just a generic comment, so please don’t interpret it as being directed towards you, but one does wonder if there are inducements for the investigator to more avidly enroll based on reimbursement, because we certainly have to support our clinical enterprise. CALKINS: So we — you know, there’s a lot published on afib ablation, but if you look at how it was collected and how much monitorin was done for asymptomatic and afib, and if they did it, none of the studies tell you what the compliance was to the monitoring protocol. So I think you’re just asking fo trouble with this objective performance criteria, unless you pick 20 percent as your target efficacy or something like that. So I think that would be a very poor approach. And the bigger challenge, which I think the group should comment on, which I think we struggle with is the issue of asymptomatic afib. And the guidance document now says that the goal should be elimination of symptomatic afib. So if you take the extreme patient, which we’ve seen in prior studies, they show up in paroxysmal afib. You do an ablation procedure. They come back six months later in permanent afib but they’re asymptomatic. And according to the current guidance document, that’s successful. The patient’s asymptomatic. They have no symptomatic afib. It’s a success. But hopefully everyone on the panel would say if you went in with an intention of getting rid of afib and now you have permanent afib, it’s hard to call that a success. And yet the primary end point of all these studies says that patient’s a success. And we all know about placebo effect you know, it’s the same thing if you go into a late afib and you end up with a left atrial flutter that’s incessant, you could call that successful because afib’s gone. Now you have an iatrogenic left atrial flutter. And prior studies that have been published have called that patient successful. DOUGLAS PACKER, MAYO Clinic: all studies of A.F. ablation should include a complete reporting of major complications which is actually not done currently. DR. MORRISON: Well, I would just like to ask the other members of the panel if any of them are as shocked as I am to hear the FDA say we’re designing trials where the sample size is based on safety rather than efficacy. I can’t think of a procedure in the history of medicine where we’ve gone to patients and say this is very expensive, it’s very dangerous, we have no idea what good it does you, but we’d like to do it, and if we can talk you into a trial we’re just going to see how many of you have serious adverse events… And to put it bluntly, as a non E.P. person, I’m just anxious to give you all enough rope to hang yourself, because I think what you’ll demonstrate — what is likely that you will demonstrate in low-risk people wh0 have lots of symptoms is that it’s very hard to demonstrate, even compared to beta blockers and calcium blockers, that ablation changes life very much. DR. KOCHERIL: Quite frankly we don’t know. I think the big picture here is that we got good results. We got symptomatic AF episode reduction and I think we were doing some good. The animal data is very helpful. It shows that adequate transmural contiguous lesions can be delivered with this catheter system employed in the fashion we were using it in the clinical trial. But aside from telling you that that was what was looked for, there’s no good way to confirm that it confirms an adequate lesion. *************** CALKINS
Understanding the Expert Consensus Recommendations on AF Ablation: Impact on Clinical Practice and Patient Care
this document will allow them to very quickly get through the learning curve and be able to start at a fairly high level instead of having to make mistakes trying to figure out some of these things on their own. All of us have heard of terrible outcomes following AF ablation, partly due to lack of physician awareness. We wanted to get the physician community up to a standard level of practice as quickly as possible to reduce the painful learning curve and the risk of patient complications. the field of AF ablation is relatively young, there’s not sufficient data published from large studies to develop a detailed guideline. the procedure has very significant risks, a 2%-6% major complication rate — even higher in some literature. And some of the complications are lethal. If a physician does an AF ablation as a first-line treatment in a 35-year-old patient, and an esophageal fistula develops and the patient dies, the physician is going to feel pretty bad about that. They will wonder why they didn’t try a drug first. So this is an acknowledgment that with this procedure, death and stroke are both very real complications. It’s not acceptable anymore to say ‘we had an 80% success rate’ and then only in the fine print somewhere in the document disclose that 40% of patients required two procedures. http://www.medscape.com/viewarticle/558137_3 (2007) HUGH CALKINS: “In contrast to catheter ablation of accessory pathways and atrioventricular nodal reentrant tachycardia, for which detailed mapping is necessary to identify appropriate sites for energy delivery, sites for catheter ablation of atrial flutter and atrial fibrillation, for example, are identified almost entirely on an anatomic basis. Although the feasibility of anatomybased catheter ablation has been demonstrated with standard catheter ablation techniques, these procedures are extremely time-consuming, require prolonged fluoroscopy exposure, and have been associated with a high incidence of complications.”http://circ.ahajournals.org/cgi/reprint/102/6/698.pdf “Our goal, and [that of] everybody involved in atrial fibrillation ablation, is to develop a safe and effective procedure that can be applied broadly to patients worldwide who have paroxysmal and persistent atrial fibrillation,” said Calkins. “Our hope is that within the next five years these procedures will be associated with long-term success rates greater than 90% and complications rates less than 1%.”http://www.theheart.org/article/789667.do “Heart rhythm societies develop consensus statement on catheter and surgical ablation of AF” 2007 J Marcus Wharton Section of Clinical Cardiac Electrophysiology, Duke University Medical Center, Durham, North Carolina, US “Furthermore, the procedures are technically difficult, arduous, time-consuming, and are not cost-effective. Given the risks of serious complications, even in experienced hands, a loud note of caution must be expressed concerning widespread application by individuals who are inexperienced in technical aspects of the procedure… “ Current Controlled Trials in Cardiovascular Medicine 2001, 2:67-70 http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=59627
*** Guidelines for supervisor presence at at stress test, what about ablation? http://circ.ahajournals.org/cgi/reprint/102/14/1726.pdf COMPLICATION RATES AT HOPKINS: All patients (n = 517) undergoing catheter ablation for AF at Johns Hopkins Hospital between February, 2001 and June, 2007 were prospectively enrolled in a database. Data from 641 consecutive procedures were analyzed and complications considered if they occurred within 30 days of ablation. Major complications were defined as those that required intervention, resulted in long-term disability, or prolonged hospitalization. Results: Thirty-two major complications occurred in 641 procedures (5%). Among the patients with major complications, seven had cerebrovascular accident (CVA), eight had tamponade, one had PV occlusion with hemoptysis, and 11 had vascular injury requiring surgical repair and/or transfusion. No periprocedural deaths occurred, and no instances of esophageal injury were seen. Complication rates were higher during the first 100 cases (9.0%) than during the subsequent 541 (4.3%). CALKINS Journal of cardiovascular electrophysiology 19(6):627-31, 2008 Jun Hugh Calkins told Pam and me that there had never been any complications with the procedure at Hopkins. His report above states that there were 641 procedures in 65 months. That’s roughly 10 per month. If procedures began in Feb ’01 and Pam had her procedure in March ’02, that means that 130 procedures were done in the 13 months before Pam’s. Calkins says the complication rate was 9% during the first 100 cases, meaning that there would have been at least 11 complications with this procedure before Pam had hers. Who signed off on buying the biosense webster ablation system? “Today it can take $60, $80, $100 million, or more to get a PMA-based medical device company to cashflow positive. If the public market is not available, where does that money come from? As companies look to complete large late-stage rounds of $25-40 million, CEOs increasingly are looking to privateequity for investment dollars. What is private equity and how do you access it? At what stage does acompany become an attractive investment for a private equity or hedge fund? Join a CEO and severalprivate equity investors as they discuss how to identify these important late-stage players and how tounderstand what it takes to get a funding commitment” http://www.docstoc.com/docs/3905699/TUESDAY-JUNE-p-m-WEDNESDAY-JUNE-a-m-p-m http://www.wsgr.com/WSGR/Index.aspx http://www.fda.gov/ohrms/dockets/ac/07/briefing/2007-429 “I think all of us are aware of the fact that the published literature probably tremendously overestimates the true efficacy of catheter ablation…” Hugh Calkins http://www.fda.gov/OHRMS/DOCKETS/ac/07/transcripts/2007-4318t2-02.pdf “These trials tend to be small ones, at single medical centers. They may be aimed at polishing a doctor’s résumé or making a center seem at the vanguard… Others studies, by companies, are designed to persuade doctors to use their drugs.” NYT CANCER trials… http://www.nytimes.com/2009/08/03/health/research/03trials.html?ref=todayspaper ************************************ I strongly suspect that David Erdman is the figment of some copywriter’s imagination – but if he does exist, I’d be curious as to his current condition, because ablation of the inside of the pulmonary veins was abandoned after practitioners ran in to an “unforeseen complication” called pulmonary vein stenosis. Basically, the veins that supply blood to the heart become occluded and start to close off. In fact Hugh Calkins was one of the earliest to sound the alarm: He wrote this in 2001: ” … And a final obstacle was the growing appreciation that pulmonary vein stenosis may occur as a complication of catheter ablation within the pulmonary veins…” And he told this to the FDA in 2003, the same year he was enticing patients with the Dave Erdman success story: “What we’ve learned obviously as we look back, years ago we were ablating deep into the pulmonary veins creating all this pulmonary vein stenosis thinking we were doing good. At the end of the day, a lot of people were stepping back and saying ‘We have to be out of the pulmonary veins for that.” Calkins may have been stepping back and telling colleagues what he really thought, but he certainly was not telling patients what he really thought. Eventually, Calkins backed off his claims for a cure altogether — going so far as to suggest the word “cure” be banned in the literature *** Catheter Ablation of Afib: Two Techniques Compared: http://cardiology.jwatch.org/cgi/content/full/2004/123/2 Commentary on Oral Remarkable advances have been made recently in catheter ablation techniques for atrial fibrillation (AF). In fact, 2 techniques that specifically target the pulmonary veins (PVs) have had favorable results. Segmental ostial ablation involves electrical isolation of targeted segments of the PV ostia. With circumferential ablation (also known as left atrial ablation), the PVs are completely encircled electrically. In a randomized trial, researchers compared the 2 techniques in 80 consecutive patients (mean age, 52) with symptomatic paroxysmal AF. Patients with left atrial size >55 mm were excluded. Segmental procedures were guided by a lasso catheter, whereas circumferential procedures were guided by an electroanatomic mapping system. Procedure duration did not differ significantly between the 2 groups; fluoroscopy duration was shorter in the circumferential group, but not significantly so. By 6-month follow-up, significantly more patients in the circumferential group (88%) than in the segmental group (67%) were free of symptomatic paroxysmal AF without taking antiarrhythmic drugs. Repeat procedures were necessary in 18% of the segmental group and 0% of the circumferential group. The only complication was left atrial flutter in 1 patient in the circumferential group. Comment: In this first randomized comparison of circumferential ablation with segmental ostial ablation, the circumferential technique was more effective in keeping patients free of paroxysmal atrial fibrillation for 6 months. Although the positive results bode well for the circumferential technique, we must remember that long-term success has yet to be established and that the potential for serious complications is real (in most series, 0.5% to 1% each for stroke, PV stenosis, and cardiac tamponade). For now, only patients with highly symptomatic paroxysmal AF who have failed at least 1 antiarrhythmic drug should be considered for catheter ablation using either of the 2 tested procedures. — Hugh Calkins, MD Published in Journal Watch Cardiology January 23, 2004 ********************************************* The American Medical Association Council on Ethical and Judicial Affairs “Situations occasionally occur in which a patient suffers significant medical complications that may have resulted from the physician’s mistake or judgment. In these situations, the physician is ethically required to inform the patient of all facts necessary to ensure understanding of what has occurred….
A physician who uncovers evidence of major errors by colleagues or identifies possible flaws in medical devices faces an ethical dilemma. Such situations may arise when a physician witnesses an error or flaw directly, or when a patient is referred by a colleague or third party for corrective treatment. Physicians are ethically obliged to facilitate disclosure to individual patients; they also should report new and serious medication-related adverse events and possible medical device defects to the relevant regulatory agencies and manufacturers. But when should a physician report previously undocumented problems at professional meetings or in peer-reviewed journals? Currently, no published ethics guidelines mandate a physician to publicly disclose adverse events or device flaws.
An individual physician generally sees only a small percentage of patients treated with a specific medication or medical device. Isolated physicians often have difficulty proving a causal relationship between the adverse event and a medication because individual physicians rarely have sufficient data for meaningful statistical analysis. Publication of poorly supported suspicions or opinions may inappropriately malign valuable procedures, medications, or devices. Even vague and unsupported suspicions may have dramatic commercial repercussions for a device manufacturer or biotechnology company. Physicians may be reluctant to publish unfavorable findings because of the lack of definitive proof, fear that unsupported disclosure will lead to libel suits, and concern about undermining professional relationships with colleagues or medical companies…. Disclosure of serious medical errors to patients generally is the best ethical and clinical course. Patients have a fundamental . Furthermore, most major errors ultimately are exposed with or without physician disclosure, and patients are more likely to be aggrieved and to sue physicians who are perceived as deceitful.… The American Medical Association Council on Ethical and Judicial Affairs states, “Concern regarding legal liability which might result following truthful disclosure should not affect the physician’s honesty with a patient.”
The fear of damage to reputation and loss of respect from peers may also inhibit physicians from disclosing errors. Error disclosure to peers must be recognized and accepted as a fundamental part of a comprehensive error-reduction program. Guidelines should be created that describe when physicians should disclose medical errors, particularly system-wide errors. The guidelines should also describe a course of action when one identifies errors made by others (including directly notifying the physician in error) or describes an error he or she has made. In particular, physicians-in-training must be notified in such a way that helps maintain their confidence and professional development…. Similarly, institutions prize their reputations, and nonstatutory reporting of medical errors is unlikely.
http://www.chestjournal.org/content/131/3/890.full And, and I wouldn’t be surprised that, in the future, we continue those types of efforts, where we may be coming to you a little bit more informally, asking for your good clinical, as well as pre-clinical, opinions on various issues of clinical design that we might be struggling with at the time. I think that being able to air some of those concerns, as well as having input from industry and the public, helps to put them in the forefront, so that when we sit down and we actually do a lot of the behind-the-scenes work that’s not necessarily out in the open, we’re able to have a little bit of a more level footing when we’re dealing with the individual manufacturers. So, that’s currently where those efforts are. http://www.fda.gov/OHRMS/DOCKETS/AC/00/transcripts/3628t2.rtf
**********************
The law requires that ordinary citizens be allowed to comment during the approval process. Unfortunately, not many ordinary citizens exercise their rights to attend. http://www.fda.gov/OHRMS/DOCKETS/AC/00/transcripts/3628t2.rtf***** 1999 was a busy year for Calkins. In addition to the Cardima work, we was a Principle Investigator in at least 14 other projects. St. Jude Medical was testing out a new Implantable Defibrillators in nonischemic cardiomyopathy,” the PI for “Evaluation of high density array catheters in patients with ventricular tachycardia (Cardiac Pathways) PI for “Low energy safety study” (LESS): Efficacy of Ventricular defibrillation with low energy margins (CPI) (P.I. H. Calkins) Guidant ICDs Cardiac Pathways was running a study to evaluate catheters in with ventricular tachycardia (Cardiac Pathways) Co-investigator, “An evaluation of radiofrequency ablation in the right atrium for treatment of atrial fibrillation” (P.I. H. Calkins) Co-investigator, “Monophasic vs. biphasic waveforms for ventricular fibrillation” (Zoll) (P.I. H. Calkins) Co-investigator, “Monophasic vs. biphasic waveforms for atrial fibrillation” (Zoll) (P.I. H. Calkins) 1997- 1999 Co-investigator, Co-investigator, Co-investigator, “Feasability of using a multi-electrode catheter in the Coronary veins for epicardial mapping of ventricular tachycardia: Implications for RF catheter ablation “ (P.I. H. Calkins) Co-investigator, Co-investigator, “Sudden cardiac death in heart failure trial” (SCD-Heft) (NIH and Medtronic) (P.I. H. Calkins) Co-investigator, “ Linear-phased radio-frequency ablation system “HRT” (CPI) (P.I. H. Calkins) Co-investigator, “Dynamic over-drive pacing for the prevention of atrial fibrillation” (ADOPT A and B)(St. Jude Medical) (P.I. H. Calkins) Co-investigator, “The North American Vasovagal Pacemaker Study” (North Western University) (P. I. H. Calkins) 1998-1999 Co-investigator, “PhaseII-Evaluation of the Cardima revelation treatment microcatheter for the treatment of atrial fibrillation” (P.I. H. Calkins) Co-investigator, “Clinical investigation of the CPI Endotak Endurance EZ defibrillation system” (P.I. H. Calkins) Co-investigator, “Ventak CHF AICD Biventricular Pacing Study” (P.I. H Calkins) ***************************
Berger Pathfinder: Cardima Successfully Treats First Patient in United States Atrial Fibrillation Study at the Johns Hopkins Hospital. http://www.thefreelibrary.com/CARDIMA+REPORTS+105%25+INCREASE+IN+REVENUES.-a053249045
Calkins Guidant 1999 linear lesions http://www.ncbi.nlm.nih.gov/pubmed/10089870 ***** “One thing is evident: many strategic and practical questions need to be answered before this approach is to be considered an established therapy.” Editorial 2004 The European Society of Cardiology http://europace.oxfordjournals.org/cgi/reprint/6/2/79.pdf ***** Cardima , a Fremont, Calif., medical-device company, almost doubled its market value, surging 2 13/32, or 91.7%, to 5 1/32. Cardima said it received regulatory approval to begin selling its Revelation Tx atrial fibrillation microcatheter in the European Union.http://online.wsj.com/article/SB912777708109922000.html?mod=googlewsj Dec 4, 1998 ******* Nov 18, 2004 Cardima Announces Receipt of Notice From Nasdaq Fell below $1 gets warning. http://findarticles.com/p/articles/mi_m0EIN/is_2004_Nov_18/ai_n6366383/?tag=content;col1 ********************** December 2003 StockPickReport.Com announces stock evaluation ratings on Hecla Mining, Anheuser-Busch, Cardima Inc, Compuware Corp, Continental Airlines.http://findarticles.com/p/articles/mi_hb5243/is_200312/ai_n19961026/?tag=content;col1 M2 Presswire, December, 2003 StockPickReport.Com announces stock evaluation ratings on Hecla Mining, Anheuser-Busch, Cardima Inc, Compuware Corp, Continental Airlines(C)1994-2003 M2 COMMUNICATIONS LTD RDATE:12022003 SHREVEPORT, La. — StockPickReport.Com (IARD#119079 – makes these short-term stock recommendations: Hecla Mining Co (NYSE:HL) – WEAK BUYAnheuser-Busch Cos Inc (NYSE:BUD) – SELLCardima Inc (Nasdaq:CRDM) – ****** **************** Conclusion: Published success rates are much better than current successrates in a large single centre. It is possible that the informationregarding outcome given to patients during the consent processis not accurate. EuroPace 2007 “It would be nice to know that the thousands of people that are having this procedure done every year are having it done for a good reason…. Most of the data that are out there discuss symptomatic improvement, and these are largely observational experiences, with no blinding and no randomization involved,” FDA medical officer Dr Randall Brockman told heartwire. “When you talk about improvements in quality of life or reductions in symptomatic episodes of atrial fibrillation, it’s a little hard to be sure that you’re seeing a treatment effect and not the effects of placebo. Placebo can be very powerful. We learned that from other therapeutic lines, and so we’re very sensitive to it. Catheter ablation may be very helpful and the jury is coming in, but it’s not in yet.” 2005 http://www.theheart.org/article/546039.do “A rapidly developing therapy that relies on both recent technologies and evolving techniques…” Hugh Calkins 2002 Catheter Entrapment in the Mitral Valve Apparatus…” Adminisphere
editing…
“This Never Happened Before”
He wrote this about Pam’s procedure: “A review of the literature reveals that catheter entrapment in the mitral valve has been reported in association with catheter ablation procedures.” He cites two cases. I found a few more — and it wasn’t very difficult. To quote Hugh Calkins himself: “Because the nature of complications for cardiac catheterizations is similar, the same format for presenting complications is used to summarize theses articles.” 1991 “Aortic valve leaflet perforation during radiofrequency ablation.” PACE Seifert MJ, Morady F, Calkins HG, Langberg JJ. Division of Internal Medicine, University of Michigan Medical Center, Ann Arbor 48109. http://www.ncbi.nlm.nih.gov/pubmed/1721146 1992: “One patient developed valvular damage as a conse-quence of catheter trauma. The patient was noted to…other complications resulted from catheter placement and manipulation. Hugh Calkins, Circulation 1992;85;1337-1346 1993 “In such a situation, the catheter should be carefully manipulated in order to avoid entrapment into the mitral valve apparatus.” Hindricks G: (MERFS): complications of radiofrequency catheter ablation of arrhythmias. Eur Heart J 1993, 14:1644-1653. 1994 “Catheter entrapment in the mitral valve apparatus during radiofrequency ablation. Conte, Geiser, Curtis, Pacing Clin Electrophisiology 17:1681 1994“Complications associated with radiofrequency catheter ablation… Valve damage.” Annals of Internal Medicine
1997 The following potential adverse events are applicable to all catheterization and ablation procedures in general and are not dependent on catheter type: … valvular damage. … Complications associated with cardiac catheterization have been reported in the literature… valvular damage.” http://tinyurl.com/CordisWebster-IFU 1998 “We describe a patient with Wolff-Parkinson-White syndrome in whom a catheter became entrapped in the mitral valve apparatus during radiofrequency ablation. Pacing Clin Electrophysiol.Apr;21(4 Pt 1):772-3. 1999 Calkins report of valve damage during catheter ablation : (Circulation. 1999;99:262-270.) 1999 “Certain risks are associated with RF ablation. They includethe general risks of any cardiac catheterization, such as… valvular damage” Hein J. J. Wellens, MD http://circ.ahajournals.org/cgi/content/full/99/2/195 w/editorial specifically citing Calkins: http://circ.ahajournals.org/cgi/content/full/99/2/262) 1999 “Adverse events which may be associated with catheterization and ablation include …valvular damage.” Cardiac Pathways Chilli Cooled Ablation System Information for Use, 1999: http://www.fda.gov/cdrh/pdf/P980003c.pdf 2000 “… Damage to the mitral valve apparatus from cathetermanipulation canoccur.” http://heart.bmj.com/cgi/content/full/84/5/553 2000 “Serious complications can occur and include valvular disruption.” American College of Cardiology http://circ.ahajournals.org/cgi/content/short/102/18/2309 2001 “Complications associated with catheter ablation… may result from catheter manipulation valvular damage…” Hugh Calkins 2001;85;594-600 Heart 2001 Cardima Evaluation Study for Revelation Catheter 2001, citing work by Hugh Calkins, who was employed by the company to work on the study. “Anticipated Adverse Effects: Valve Damage” http://www.fda.gov/ohrms/dockets/ac/07/briefing/2007-4297b1_16%20-%20APPENDIX%20A%20Study%20Protocol.pdf 2001 Complications associated with catheter ablation… valvular damage… may result from catheter manipulation. Hugh Calkins: http://heart.bmj.com/cgi/content/full/85/5/594 2002 Cardima REVELATION™Tx Microcatheter System and NavAblator™ Ablation Catheter Evaluation of Radiofrequency (RF) Ablation for Atrial Fibrillation in the Right Atrium Anticipated Adverse Effects Possible adverse effects that may be anticipated in association with the investigational devices and procedure : Valve or cardiac structure damage” – Hugh Calkins Next Chapter: This has nothing to do with the story, but it’s interesting. A transcript synopsis of a meeting that was held on 9/11. ***** ********** (In the medical literature, Hugh Calkins always confirms what Jeff Brinker wrote in 1991 about cardiac catheterization in general: The experience and knowledge of the performing physician ————-
Medical experiment disclosure hinges on a flawed honor system Hopkins worker death raises wider questions.
By Tom Pelton, Sun Staff, August 12, 2001 Problems at Hopkins Dr. Greg Koski, director of the federal Office of Human Research Protections, said he doesn’t know how accurate Shamoo’s figures might be, but he acknowledges that the underreporting of “adverse events” could be a problem. Koski’s agency recently suspended most experiments at Johns Hopkins when it found systemic problems with the review of experiments after the death June 2 of volunteer Ellen Roche. Koski said his agency will work with the National Institute of Health and the Food and Drug Administration this fall to improve the national system for monitoring experiments and collecting and sharing reports of deaths and injuries. “It’s difficult to know how much is underreported,” Koski said. “Many of these adverse events are being handled at the local level, and I don’t know if they are being handled in the optimal way. There is no question that there is room for improvement.” Koski added, however, that federal law does not require researchers to report all injuries and deaths among study subjects to his agency. It requires reports only of regulatory violations and health problems that are unexpected and likely a result of the treatment. The agency leaves it up to researchers and university review boards to sort through the sticky problem of separating which health problems are a product of illnesses and which are side effects of the drugs. Koski’s agency, with only 45 employees, would be overwhelmed with paperwork if every research institution in the United States sent in every report of problems in the thousands of federally funded experiments across the country, said Bill Hall, a spokesman for the agency. The number of incident reports flowing into the agency has almost tripled in recent years, rising from 100 in 1997 to 290 in 2000, with at least a third of these detailing unexpected health problems suffered by volunteers, according to the agency. The increase stems from increasing awareness of federal reporting requirements and a surging amont of medical research, Koski said. In contrast to Johns Hopkins, the University of Maryland released its adverse-events numbers when asked by The Sun. The review boards that monitor experiments at the university’s medical school received 880 reports of “serious adverse events” to volunteers during more than 1,000 experiments last year. The university defines “serious adverse events” as “any untoward medical outcome occurring in the context of research” – which could include anything from vomiting to the deaths of seriously ill cancer or cardiac patients, according to school spokesman Larry Roberts. The majority of these health problems, in 728 cases, were judged to be unrelated to the studies – for example, volunteers injured in car accidents while away from the hospital, Roberts said. The university reported only two cases to the federal agency because they were the only cases that were unexpected and probably linked to the treatment, and not to an underlying illness, Roberts said. One was a blood infection that a researcher mistakenly gave to a 24-year-old volunteer in a metabolism study. Another was the death of a 61-year-old man with life-threatening heart disease who may have suffered a reaction to medications he was taking in a study, Roberts said. The Johns Hopkins University, unlike Maryland, refused to release information about the number of problems suffered by volunteers in its more than 2,700 experiments last year. Joann Rogers, a spokeswoman for Hopkins, said the university has no evidence of widespread problems with underreporting. “We are looking to see if there are systemic problems,” Rogers said. “If there are, we are going to do whatever it takes to change that.” Shamoo and others complain that self-policing invites a lack of candor. “It’s an honor system,” said Arthur Caplan, director of the University of Pennsylvania’s Bioethics Program. “Many adverse events do not get reported because doctors and researchers don’t like to think about themselves causing harm. So if there’s something else to blame it on, like an illness, they will.” “Few Decisions bespeak greater trust and confidence than the decision of the patient to proceed with surgery. Implicit in that decision is a willingness of the patient to put his life or her life in the hands of a known and trusted medical doctor… the doctor who, without the consent of the patient, permits another surgeon to operate violates not only a fundamental tenet of the medical profession, but also a legal obligation.” Supreme Court of New Jersey 92 N.J. at 463-465, 457 A.2d at 440-441. ———————– “Uh… You Weren’t There That Day” ———————- Risk Management: “You’ll Get Nothing!” ———————— The Wilmer Eye Center on Scratched Corneas: “Oh, we see a lot of that in the ICU.” Catheter ablation of AF frequently requires the use of CT scan prior to the procedure and a long fluoroscopy time during the procedure. Further complicating the issue is the fact that AF ablation procedures are often done in the obese patient, increasing the exposure to patient and operator. Very low frame rate pulsed fluoroscopy systems have become the norm to minimize radiation exposure. Skin radiation “burns” with proper operating equipment are currently extremely rare http://www.medscape.com/viewarticle/558370_8 _______________________________________ draftdraft http://www.theheart.org/article/546039.do Here is some mind-bending logic: Experts say time has come for AF ablation RCTs: “Only thing missing is the data” August, 2005 “We’re missing a lot of things at this point,” Dr Hugh Calkins (Johns Hopkins University Medical Center, Baltimore, MD) told heartwire. “Everything is based on, ‘This is how I think my patients are doing.’ If history holds true, the results are always worse when the procedure is held up to a multicenter, rigorous study, where you prospectively define the complications and evaluate. We need better data on the true efficacy and safety of the procedure in patients selected as part of a multicenter study in a rigorous, prospective fashion.” Dr Andrea Natale, medical director for the Center for Atrial Fibrillation at the Cleveland Clinic, told heartwirethat the center performs five to six AF ablations every day and that the waiting list extends from anywhere between four and nine months. Smaller centers perform fewer procedures, and their success and complication rates vary, he noted. “Atrial fibrillation ablation is technically very challenging,” he said. “This is the deterrent for less skilled hands in embracing the procedure.” Kim,Calkins predicts that there is probably a two- to five-year horizon before ablation of AF is a primary therapy. “Some doctors are pretty enthusiastic about ablation as a primary therapy, but they’re only enthusiastic until a patient has a stroke or some type of devastating consequence. Then the enthusiasm tends to go down a little bit,” he notes. —————————- Nurse’s notes Kristi w/ Walkman Tom Waits Were you ever able to pin that lying little weasel Hugh Calkins down about his complication rate? Thank You, Dan Walter Dan Walter wrote: Kim Young wrote: Dear Sir, Thank you for your comments about an article on Cardiosource by Dr. Hugh Calkins, Atrial Fibrillation: Drugs or Ablation. From your coments, it seems as though your issue is with Dr. Calkins, and I recommend that you get in touch with him directly. We are, however, seeking to get clarification of the statement in question and will modify the paragraph accordingly. In the paragraph above the one quoted by you (see below) Dr. Calkins states that the complication rate for the procedure is 6%. This is clearly inconsistent with his next comment of “one-in-a-thousand”. We will ask Dr. Calkins to clarify this inconsistency for us , and correct it on the site. Sincerely, Kim Young Senior Editor, Cardiosource _____________________________________________ The Records http://well.blogs.nytimes.com/2008/06/27/the-growing-disconnect-between-doctors-and-patients/
-
140.July 2nd, 2008 5:49 pmDear Dan, (79); I apologize for mischaracterizing your quotation of the ACC guideline in your original comment (79). After reading your post, I assumed you were referring to the guidelines as pertaining to EP clinical research. After reading your account of your wife’s ordeal, I understand that your quote sums up your point beautifully. There is a small but increasingly vocal movement in EP and interventional cardiology which calls for restraint and reason in practice, particularly in a field where technologic advancement is so rapid. There is also an ever present paradox in procedure-driven fields which require intense training at well known academic centers; both the patients and the trainees go there for access to high profile practitioners. Institutions and physicians must constantly balance the care of the patient with the training of the next great, for example, electrophysiologist. As a result, all patients at these centers need to know, that 1)trainees may be involved in their care; and 2) theyhave a right to limit a trainee’s involvement if they choose. The best situation is when the trainee/fellow is involved all aspects of care-the consult, the office visit, the consent, and the follow up. It is always better to get to know the family as well-after all, this is what the the rest of their career will be like. When you get to know a patient, you tend to think of them (’how can I reduce this person’s risk and make their life better?’) before yourself (’what new technique can I try out on this patient today?’). I am convinced that this approach has led me to choose wisely, and has saved more than couple patients from complications. — Posted by Mike (84, 85)
-
84.July 1st, 2008 9:35 amDan Walter (79) brings up an interesting point. I happen to be a “research doctor” and Electrophysiogist (a Cardiologist who studies the electrical properties of the heart). I agree that there is intellectual and ethical tension inherent in clinical and basic science research. On one hand, patients have a right to get care which is shown to be efficacious and safe. The entire concept of research has evolved because in the not-so distant past, treatments were based on “good ideas” rather than solid evidence. On the other hand, in order to demonstrate clinical efficacy, one needs to perform clinical research. There is no doubt that some researchers become so invested in their trials that they lose sight of the best interest of the individual patient. This is unacceptable. I personally meet with each patient enrolled in the study, assure them that there are alternatives to my research, and let hem know that they are entitled to receive the standard of care treatment without exception if they wish. However, the excerpt you quote from the ACC/AHA guidelines misses your point entirely, and is out of context. The quoted text refers to an ongoing debate regarding education, not clinical research. The admonition is akin to reminding conservatory students that it is the music, not the recording technology, that makes their calling special. Further, the author of the quote, a well known “research” physician” in a Boston “research hospital,” is famous for putting the individual patient above all else. We cannot provide patients with the care they deserve and demand without responsible clinical research. — Posted by Mike
-
85.July 1st, 2008 10:02 amDear Dan (79), I just read your touching account of your wife’s ordeal. You have effectively captured an aspect of interventional cardiology and critical care medicine which we all wish did not exist. My heart goes out to you and your family, and you are in my prayers. My only hope is that the “lesson learned” by myself and my interventional minded colleagues is not just one of technique, but one of humility and honesty; we all (surgeons, physicians, and someties patients) tend to minimize, and sometimes forget completely, the audacity of what we are trying to do: namely, stop or alter completely a biologic process which has been evolving at least as long as we have been. When you think about it, we should be suprised that it works at all. We definitely have a long way to go. Again, you are in my thoughts and prayers. — Posted by Mike
-
112.July 1st, 2008 4:49 pmDear Mike (#84) Thanks for your comments on my story. It is very important to me that I get it right and I am curious to know more about your feelings on the AHA/ACC quote about EP technology: “… Although it is exciting, it should be kept in mind that the technology facilitates the application of those fundamental principles of Electrophysiology only for the benefit of arrhythmia patients.” I do not think I am misreading this. It appears to me to be a caution to physicians that although this new technology (enhanced catheter ablation techniques for AFIB) is fascinating – don’t forget that is being developed for the good of the patient. The fact that “the author of the quote… is famous for putting the individual patient above all else.” would seem support my interpretation. Im not sure I understand the music analogy – aside from as it applies to patient safety. I would really appreciate your thoughts. — Posted by Dan Walter
***** http://www.a-fib.com/BostonA-FibSymposium2006.htm:
“Cured” patients were found to be in A-Fib 31% of the time. 82% of these A-Fib attacks were silent (asymptomatic). (In this study 57% of patients who thought they were experiencing A-Fib symptoms were actually in normal sinus rhythm. Symptoms of shortness of breath and chest discomfort were good predictors of being in A-Fib, whereas skipped beats was a poor predictor.) Dr. Calkins suggested a different way of defining success after AF Ablation which he called “reducing the A-Fib Burden,” rather than complete elimination of A-Fib symptoms. For example, after a “successful” A-Fib Ablation a patient may go from constant (Chronic) A-Fib to occasional (Paroxysmal) A-Fib which is a “reduction of their A-Fib burden.”
Marchlinski Chilli v standard ablation catheter study http://www3.interscience.wiley.com/cgi-bin/fulltext/118574459/PDFSTART 2006.” NO Difference. Study Design: “This was a single center, patient-blinded pilot study in which participating subjects were randomized (using a 2 × 2 factorial table) to undergo EI of all versus arrhythmogenic PVs only using either an 8-mm tip (NaviStarTM Biosense Webster, Diamond Bar, CA, USA) or cooled tip (Chilli Boston Scientific, Natick, MA, USA) catheter. The study protocol and consent forms were approved by the institutional review board of the University of Pennsylvania.” ATRACURE APPEAL TEMPLATE (To be printed on the physician’s letterhead. Please insert specific evidence of medical necessity from the patient’s medical record) April 9, 2007 Coventry Healthcare of Delaware, Inc. Attention: Appeals Coordinator 2751 Centerville Road Suite 400 Wilmington, Delaware 19808 RE: Pre-Service Appeal CPT 33255 is medically necessary. Please call me at your earliest convenience to understand the numerous patient benefits. Patient: Subscriber ID#: Date of Birth: Facility: Address: Dear Appeals Coordinator: The purpose of this letter is to establish the medical necessity of a procedure that I must perform on your subscriber as soon as possible. Last week, Coventry issued a pre-service denial and I would like a board-certified cardiothoracic surgeon to review this request for reconsideration. CPT 33255 [Operative tissue ablation and reconstruction of atria, extensive (e.g. maze procedure); without cardiopulmonary bypass] is medically necessary. In view of numerous CPT coding changes that took effect on January 1, 2007, I am hopeful this pre-service denial was simply the result of a miscommunication? As you may know, the AMA released five new CPT codes in the Surgery/Cardiovascular “Electrophysiologic Operative Procedure” section of CPT 2007. I am not performing an investigational/experimental procedure. The CPT code I selected is not a Category III T-code used for tracking new and emerging technologies. I selected a fully-valued Level I CPT code recently surveyed by the Society of Thoracic Surgeons (STS) in 2006 and released by the AMA in 2007. Please consult with a cardiothoracic surgeon, the STS and/or AMA to better appreciate that tissue ablation can be accomplished by many different methods. Simplification of the maze procedure has been made possible by different ablation techniques. The acceptance of alternative energy technology that shortens and simplifies the surgical management of atrial fibrillation (AF) was the reason behind these new CPT codes. The “cut-and sew” maze CPT code 33253 was deleted in 2006 and replaced with 5 new CPT codes to better match contemporary surgical practice. While some payers continue to view the classic “cut-and-sew” Cox-maze procedure to be the surgical “gold standard”, it is very important that you fully appreciate the risks associated with this lengthy, complex and difficult procedure. The requirement for cardiopulmonary bypass (CPB) and the technical difficulty of this approach have limited its use Everyday in clinical practice, cardiothoracic surgeons create alternative lines of conduction blocks with improved technology without the known morbidity associated with a full sternotomy and CPB. If Anthem BCBS, the largest private payer in the U.S, considers this CPT code and ICD-9-CM Procedure Code 37.33 (excision or destruction of other lesions or tissue of heart open approach/ trans-thoracic approach) to be medically necessary for drug resistant atrial fibrillation or flutter, then so should you. Anthem’s medical policy for the Maze procedure is attached for your review and consideration. My surgical plan for your subscriber is to use an ablative device that delivers targeted bi-polar radiofrequency energy to create discrete linear transmural lesions. Contrary to your maze medical policy, I am NOT performing a catheter ablation! Your medical policy is not in step with contemporary cardiovascular surgical practice for the treatment of persistent AF. It is outdated and in need of immediate revision. For example, it currently identifies the deleted maze CPT code 33253 as a covered benefit. Besides reviewing CPT 2007, please consult with a board certified cardiothoracic surgeon and/or me for a peer-to-peer discussion of the references cited on the enclosed bibliography. Your subscriber needs surgery now! Early intervention will increase the likelihood of restoring this patient to normal sinus rhythm. The most significant predictor of long-term AF recurrence is the duration of pre-operative AF. While the classic cut-and-sew maze procedure is extremely effective, it has been supplanted by newer operations that rely on alternate energy, such as radiofrequency, to create lines of conduction block In a systematic review of the surgical treatment of AF, Khargi et al (2005) could not identify any significant difference in the post-op sinus rhythm conversion rates between classic “cut & sew” Cox-Maze technique that requires an open sternotomy versus alternative energy sources, such as radiofrequency, which simply requires trans-thoracic incisions. The surgical objective through an open sternotomy with CPB or trans-thoracic incisions is the same – to interrupt the aberrant atrial conduction pathways in the heart that are causing the patient’s atrial fibrillation. The expected outcomes from either approach is to restore normal sinus rhythm and prevent ischemic stroke. Availability of alternative energy sources to create lesions sets has virtually eliminated the need for the cut-and-sew Cox-maze procedure. The clinical and economic gains associated with avoiding a full sternotomy and CPB are quite significant to me, my patient, and your health plan. CLINICAL JUSTIFICATION Atrial fibrillation (AF) is the most commonly occurring cardiac arrhythmia. It affects more than 2.5 million people in the United States, and its prevalence rises with age. It is associated with numerous cardiac morbidities, decreased quality of life and decreased survival. Symptoms include palpitations, decreased exercise tolerance and dyspnea. Stroke is the most feared complication of atrial fibrillation. It is well-known that patients with AF are five times more likely to suffer a stroke than patients in normal sinus rhythm. Among patients with AF, there is a 5% annual risk of stroke. Per 2006 ACC/AHA/ESC Practice Guidelines for the “Management of Patients with Atrial Fibrillation”, the inconsistent efficacy and potential toxicity of antiarrhythmic drug therapies have established the need for non-pharmacologic treatments in patients with persistent AF who fail to respond to anti-arrhythmic drug therapy. Your subscriber is an ideal candidate for an operative tissue ablation through a trans-thoracic approach (ICD-9-CM Procedure code 37.33), but as shown below, time is of the essence for this patient’s well-being. SUBSCRIBER’S MEDICAL NECESSITY (Please insert specific information about the patient, such as age, chief compliant, current medications, significant events in the past medical history, employment status, family issues). For example, this is a 46 year old independent contractor, who has suffered with AF for more than 5 years despite taking numerous anti-arrhythmics. While this patient recognizes the need for surgery, he can not afford to be out-of-work for 8-12 weeks following an open surgical procedure. With a trans-thoracic approach, I anticipate he can return to work for within 2-3 weeks. Upon your review of the enclosed NEW evidence, please do not hesitate to call me with any further questions to better appreciate the medical necessity of this surgery. I would be very happy to share additional clinical information, as well as provide further evidence regarding the effectiveness of operative tissue ablation and reconstruction of the atria through a trans-thoracic incision. In advance, thank-you for your time and re-consideration. At your earliest convenience, I await your reply in writing. Sincerely, Name of Surgeon Phone: Citations in the peer-reviewed literature that establish the medical necessity of CPT 33255 Barnett SD, and Ad N. Surgical ablation as treatment for elimination of atrial fibrillation: a META analysis. J Thorac Cardiovasc Surg 2006;131:1029-35. Benjamin EJ, et al. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998 Sep 8;98(10):946-52. Cox JL. The surgical treatment of atrial fibrillation. IV. Surgical technique. J Thorac Cardiovasc Surg 1991 ;101 :584-92. Doukas G, et al. Left atrial radiofrequency ablation during mitral valve surgery for continuous atrial fibrillation: a randomized controlled trial. JAMA 2005 Nov 9;294(18):2323-9. Fuster V, et al. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation. JACC 2006;48(4):e149-246. Gaynor SL, et al. Surgical treatment of atrial fibrillation: predictors of late recurrence. J Thorac Cardiovasc Surg 2005 Jan;129(1):104-11). Gaynor SL, et al. A prospective, single-center clinical trial of a modified Cox maze procedure with bipolar radiofrequency ablation. J Thorac Cardiovasc Surg 2004 Oct; 128(4):535-42. Gillinov AM and Saltman AE. Ablation of atrial fibrillation with concomitant cardiac surgery. Semin Thorac Cardiovasc Surg. 2007 Spring; 19 (1): 25-32. Gillinov AM. Advances in surgical treatment of atrial fibrillation. Stroke. 2007 Feb; 38 (2 Suppl): 618-23. Gillinov AM et al. Surgery for permanent atrial fibrillation: impact of patient factors and lesion sets. Ann Thorac Surg. 2006 Aug; 82 (2): 502-13. Gillinov AM, Wolf RK. Surgical ablation of atrial fibrillation. Prog Cardiovasc Dis. 2005 Nov-Dec;48(3):169-77. Gillinov AM. Ablation of atrial fibrillation with mitral valve surgery. Curr Opin Cardiol. 2005 Mar;20(2):107-14. Gillinov AM, et al. Stapled excision of the left atrial appendage. J Thorac Cardiovasc Surg 2005 Mar;129(3):679-80. Gillinov AM, et al. Surgical ablation of atrial fibrillation with bipolar radiofrequency as the primary modality. J Thorac Cardiovasc Surg. 2005 Jun;129(6):1322-9. Gillinov AM, McCarthy PM. Advances in the surgical treatment of atrial fibrillation. Cardiol Clin. 2004 Feb;22(1):147-57. Gillinov AM, McCarthy PM. Curative surgery for atrial fibrillation: current status and minimally invasive approaches. Expert Rev Cardiovasc Ther. 2003 Nov;1(4):595-603. Gillinov AM, et al. Contemporary treatment for atrial fibrillation. Pacing Clin Electrophysiol. 2003 Jul;26(7 pt 2):1641-4. Gillinov AM, McCarthy PM. Atricure bipolar radiofrequency clamp for intraoperative ablation of atrial fibrillation. Ann Thorac Surg 2002 Dec;74(6):2165-8. Gillinov AM, Blackstone EH, McCarthy PM. Atrial fibrillation: current surgical options and their assessment. Ann Thorac Surg. 2002 Dec;74(6):2210-7. Hart RG, Halperin JL, et al. Lessons from the stroke prevention in atrial fibrillation trials. Ann Intern Med. 2003 May 20; 138(10):831-8. Khargi K et al. Surgical treatment of atrial fibrillation: A systemic review. Eur J Cardiovasc Surg. 2005; 129 (1) 104-111. Lemery R, Guiraudon G. Catheter and surgical ablation strategies in atrial fibrillation: what have we learned? Curr Opin Cardiol. 2005;20(1)26-30. Misaki T et al. Recent topics on the surgical treatment for atrial fibrillation. Ann Thorac Cardiovascular Surg. 2004; 10 (5):277-280. Mokadam NA, et al. A prospective multicenter trial of bipolar radiofrequency ablation for atrial fibrillation: early results. Ann Thorac Surg 2004 Nov;78(5):1665-70. Pruitt JC, et al. Totally endoscopic ablation of lone atrial fibrillation: initial clinical experience. Ann Thorac Surg2006 Apr;81(4):1325-30.
Fuster V, et al. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation. JACC 2006;48(4):e149-246. ****** Johns Hopkins University Will Pay $800,000 To Resolve Medicare Fraud Case: Office of the Inspector General HHS: http://oig.hhs.gov/publications/docs/press/2003/021403release.pdf “cozy relationship” autism device maker hopkins: 1992 http://oig.hhs.gov/oas/reports/phs/c9000009.pdf *******
Patient stories:
Full Text Pulmonary Vein Stenosis after Catheter Ablation of Atrial Fibrillation: Emergence of a New Clinical Syndrome Ann Intern Med April 15, 2003 138:634-638 www.annals.org ********* The challenge of ablating in the human heart… (Dr. John M Blog):
Some very sad words from the comments section of a previous post on atrial fibrillation…
Dear Anonymous, I am very sorry for your loss. Making many ablation lesions in the left atrium confers significant risk. Your tragedy highlights the dilemma of medical decision making. Indeed, AF ablation is often successful, but there is risk, and complications can be life-altering or life-ending, as your words describe. We ablators struggle with this balance of information. We have to inform our patients of the risks, and these words of admonishment should be clear. However, patients can be scared out of a potentially curative procedure if presented with a litany of disasters in an un-elegant manner. Herein lies the delicate balance of treating atrial fibrillation –a highly symptomatic, but not immediately life threatening disease –with a potentially life threatening, but mostly safe procedure. Many years ago, a colleague spoke the words, “AF is not a life threatening disease, don’t make it one.” Complications occur and I wish they didn’t. When I have them, it changes my life, and my practice of medicine, but one thing for sure; the affected patient will be seeing more, not less, of me afterwards. Paradoxically, some of my most gratified patients are ones who have suffered procedural complications, who as a result of the adverse outcome, garnered much attention from me. These words of tragedy help us, and I am grateful you wrote them. They help us learn, and this makes us better, both as clinicians and as people. ******
THE DISTRICT OF DELAWARE: Yong v. Nemours, december 2004 The court will “view the underlying facts and all reasonable inferences therefrom in the light most favorable to the party opposing the motion.” The theory behind the informed consent doctrine is that every patient has the right and responsibility to determine whether to take the risk of the corrective surgery. It is no defense that the patient gave consent, if the consentwas not given with a true understanding of the nature of the operation to be performed, the seriousness of it, the organs of the bodyinvolved, the disease or incapacity to be cured, and the possibleresults. Dunham, 423 F.2d at 945. Barriocanal v.Gibbs, 433 A.2d 1051, 1172 (Del. Super. Ct. 1981).
IN THE COURT OF SPECIAL APPEALS OF MARYLAND No. 462
September Term, 1998
___________________________________
DEBORAH M. BELIN
v.
LENOX DINGLE, JR., ET AL.
___________________________________
Murphy, C.J.,
Davis,
Harrell,
JJ.
___________________________________
Opinion by Murphy, C.J., Concurring and Dissenting Opinion by Harrell, J. Filed: June 30, 1999
According to the Judicial Council of the American Medical Association, to have another physician operate on one’s patient without the patient’s knowledge and consent is a deceit. The patient is entitled to choose his own physician and should be permitted to acquiesce in or refuse to accept the substitution. The surgeon’s obligation to the patient requires him to perform the surgical operation: (1) within the scope of authority granted by the consent to the operation; (2) in accordance with the terms of the contractual relationship; (3) with complete disclosure of all facts relevant to the need and the performance of the operation; and (4) to utilize his best skill in performing he operation. The patient is entitled to the services of the particular surgeon with whom he or she contracts.
The surgeon, in accepting the patient, is obligated to utilize his personal talents in the performance of the operation to the extent required by the agreement creating the physician-patient relationship. He cannot properly delegate to another the duties which he is required to perform personally. Under normal and customary arrangement with private patients, and with reference to the usual form of consent to operation, the surgeon is obligated to perform the operation, and may use the services of assisting residents orother assisting surgeons to the extent that the operation reasonably requires the employment of such assistance. If a resident or other physician is to perform the operation under the guidance of the surgeon, it is necessary to make a full disclosure of this fact to the patient, and this should be evidenced by an appropriate statement contained in the consent. If the surgeon employed merely assists the resident or other physician in performing the operation, it is the resident or other physician who becomes the operating surgeon. If the patient is not informed as to the identity of the operating surgeon, the situation is “ghost surgery.” …… I hereby authorize Dr. Dingle and/or such assistants as may be selected or supervised by him to treat the following condition(s)
Perna v. Pirozzi, 92 N.J. 446, 457 A.2d 431 (1983), the
Supreme Court of New Jersey
Few decisions bespeak greater trust and
confidence than the decision of the patient
to proceed with surgery. Implicit in that
decision is a willingness of the patient to
put his life or her life in the hands of a
known and trusted medical doctor…
the doctor who, without the consent of the patient,
permits another surgeon to operate violates
not only a fundamental tenet of the medical
profession, but also a legal obligation.
92 N.J. at 463-465, 457 A.2d at 440-441.
Dump Beckman need records got to hopkins a raid
“Perhaps the most feared, and most lethal of the many complications that have been associated with this procedure – with mortality in excess of 75 percent.”
“ If a physician extender (e.g., physician’s assistant or nurse practitioner) or cardiology trainee is to perform any part of a procedure, this should be stated during the process of informed consent. Because the patient and physician together determine the diagnostic and treatment strategy, medical facts should be presented accurately to the patient .” American College of Cardiology Cardiac Catheterization Laboratory Standards #### While Dr. Yuh had his toes in the sand and a drink in his hand outside the Hyatt Regency Waikiki Beach Resort and Spa ($627 per person per night), I was picking through the offerings in beautiful downtown Baltimore. A decent room in Charm City, USA was going for $186.77 a night for a room with a double bed. I walked out of the Day’s Inn and fished a card out of my pocket that said Patient Relations and got in my car and went back to the hospital. Looking back, I see the question was hopelessly naive, but I had logistical problems with all these people coming to be with Pam, and so I had to ask. Pam’s son, her daughter, her mother, her sisters, her stepfather — all these people needed places to stay. They could do hotels for a while, but there was no end in sight here. I went into the office with the idea that when something like this happens they probably had some deal with the local hotels for discount vouchers – or something. They gave me some vouchers — for free coffee down in the cafeteria. Then I heard that there was a woman who rents out apartments in the immediate area for just such purposes. She’d started the program years earlier when she arrived in Baltimore with a sick child for the hospital and no place for her to stay. So she got in touch with local property owners and became the rental agent and manager for several apartments that were let to visitors for days or weeks – or months. She didn’t seem to be getting rich off the scheme. It was said that a lot of the rental properties in the immmediate vicinity of the hospital were owned by doctors and that they kept the rents artificially high. I’m not saying that I know that to be true, but it is what I was told. While Pam’s mother went to get her sister at the airport, I arranged for an efficiency apartment near the hospital with three bedrooms – about $650 a week if I remember correctly. Calkins on Ablation: ****** Hugh Calkins 2007 : ” …it’s also by far the most dangerous procedure that electrophysiologists (EPs) perform. All of us have heard of terrible outcomes following AF ablation, partly due to lack of physician awareness. We wanted to get the physician community up to a standard level of practice as quickly as possible to reduce the painful learning curve and the risk of patient complications… You can put a patient on an anti-arrhythmic drug, and they may do well for two, three, five or ten years on anti-arrhythmic drugs… The point is that the physician needs to explain to the patient what the standard of care is, and if the patient wants other than the standard of care — that is if they want to do catheter ablation as a first-line therapy — they need to be aware that they’re taking an aggressive approach. They need to understand that approach may not be wrong, but it’s not considered standard for most patients, it’s the exception, not the rule…. Dr. Calkins: 6/6 2007 I think many physicians are very frustrated because they read in the literature that catheter ablation has an 85% cure rate and yet all the patients they refer for the procedure seem to have AF after the procedure. This document is partly for them, saying first of all that we shouldn’t use the term ‘cure’ anymore for treating AF and also telling the physician community that when we publish our results, we need to report results in a standardized fashion. You can’t report an 85% success rate when 38% of the patients had three procedures. You need to report single-procedure outcomes.” http://cme.medscape.com/viewarticle/558137_4 TINY URLS http://tinyurl.com/theidealcandidateHow did the catheter get tangled in the muscles at the base of the mitral valve, which is located in the ventricle? “The catheter was in the atrium and the leaflets became entangled—in the atrium—but the mitral valve is tethered to the ventricle.” Sure. But how did the catheter get into the ventricle? “It was in the atrium” Come on. “If the mitral valve apparatus is in the atrium and entangled with the Lasso, if you pull, you can avulse the muscle in the ventricle.”
∞
Schwartzman “If you watch what is happening to the atria when you ablate the bejeezus out of them, which is what we are doing, they swell like crazy….” http://www.fda.gov/OHRMS/DOCKETS/AC/98/transcpt/3442t2b.pdf (p60), Calkins VT Ablation 2007 “It’s often only in the fine print that we see how effective the procedure really is,” said Calkins. “We’re sweeping some of the redos under the rug, but when we’re honest and look at this objectively, we can’t be telling our patients undergoing this lengthy five- to six-hour procedure that this is going to cure them of their VT.” In addition, Calkins noted that there are risks with ablation, noting that one patient in this study died during the procedure. http://www.theheart.org/article/803555.do FREMONT, Calif.–(BW HealthWire)–July 9, 1997–Cardima, Inc. (NASDAQ:CRDM) announced today completion of the first two patients in the initial phase of a clinical trial designed to evaluate safety and effectiveness of the Cardima Pathfinder AF microcatheter system for the treatment of atrial fibrillation (AF), a condition of the heart characterized by the irregular and very rapid beating of the heart’s atria, or upper chambers, that can lead to poor blood flow and clotting, which potentially may lead to stroke. Cardima is pioneering a minimally invasive catheter-based intervention for AF, which duplicates the success of the Maze operation, a highly invasive open-heart procedure and the only known effective treatment today. The first two patients, enrolled at the Stanford University Hospital underwent electrophysiological studies to demonstrate the placement of the catheters, a prerequisite for the catheter-based treatment. Stanford’s principal investigator Ruey J. Sung, M.D., Professor of Medicine, stated that “initial results for its diagnostic use revealed that the Pathfinder AF could be readily placed in pre-selected locations of the right atrium from which high quality recordings could be obtained. The catheter also could easily pace the heart at good threshold voltages.” The first cases were completed in less than 45 minutes each.
Hi Gill just dropped into the BB after a few months layoff and seen your post. Yes you are correct I have had 5 ablations though ablation No 4 stopped the AF in its tracks over two years ago. Ablation No 5 was for Left Atrial Flutter, a side effect that can come about after a successful ablation for AF. Left Atrial Flutter can be stopped by a cardioversion and indeed in my case the arrhthmia was stopped by that proceedure however within weeks of the cardioversion I went ino episodes of Bigeminy, Trigminy and Quadgiminy arrhythmias which I believe you are familiar with. Bordeaux advised that another proceedure was necessary IF I wanted to be totally free of theses curses, hence ablation No5 Barry Steve Ryan, who runs a different website has had five ablations. I was emailing back and fourth with him, and he told me he had 3 failed ablations here in the US. He then traveled to France and had an ablation followed by a touch up ablation a couple of days later. That was back in 1998 and the last time I had talked to him a couple of months ago, he had only had one episode since 1998. Katy – I had one Natale ablation in 2003. I was afib free for a bit over 4 years but then started to have some breakthroughs… one every 6 to 9 months. It took a while for it to dawn on me that I was probably wasting potassium… was tested.. yes, some wasting and since being very diligent with keeping up with the Essential Trio supplements (magnesium, potassium and taurine) plus adding the other critial nutrients for heart energy support… ie, carnitine, coQ10, ribose, Omega 3’s and a B complex, I’ve been afib free. As a result of my success, I wrote the observational report called The Strategy and companion report to that is covered in CR 72. Since AF is the result of dietary sodium (salt) dominance over potassium which affects the ability of heart cells to regulate the energy (voltage), it is important to be sure that you are supporting your needs by dietary intake and supplements if needed. Shannon (—.hawaii.res.rr.com) Date: 07-05-11 13:22 Had one so far for persistent highly symptomatic high speed Afib/Flutter 3 years ago..At the time Dr. Natale said I would likey need one more to deal with a potential atypical left atrial flutter ciircuit they were not able to do during eht intital very long ( for him) procedure with 2 full hours of actual burn time required. I havent had on blip of AFIB since and have a pacemaker recording everything to prove that. But I have had three Left flutter episodes that I gotr cardioverted within hours each time as, alas, there is no way to get out of such an atypical left flutter with drugs or on your own. Srtill I view this as remarkable success and as long as the frequency of breakthroughs stays at teh 10 to 14 month interval, I’ll settle for an annual shock as the price for my otherwise clear and clean NSR. Author: Gill (92.20.1.—) Date: 07-05-11 12:14 Katy Search for posts with Barry G as author – I think he had 5 before he achieved nsr. I had 2 in Bordeaux, the second one was three days after the first because AF recurred. Prof. Haissaguerre thought there could be a gap in one of the lines but this was not the case. He found an extremely toxic focus in the coronary sinus. Gill (nsr for 8½ years since ablations)
| Re: Ablations – what’s most you’ve had? | |
|
______________________________
Time Magazine Ellen Roche 4/22/2002 http://www.time.com/time/covers/1101020422/story3.html ______________________ FDA Transcript Navistar Thermocool for Afib: http://www.fda.gov/ohrms/dockets/ac/08/transcripts/2008-4393-t02.pdf ____________ REALTORS CODE OF ETHICS Where the word Realtors® is used in this Code and Preamble, it shall be deemed to include Realtor-Associate®s. While the Code of Ethics establishes obligations that may be higher than those mandated by law, in any instance where the Code of Ethics and the law conflict, the obligations of the law must take precedence.
Preamble
Under all is the land. Upon its wise utilization and widely allocated ownership depend the survival and growth of free institutions and of our civilization. Realtors® should recognize that the interests of the nation and its citizens require the highest and best use of the land and the widest distribution of land ownership. They require the creation of adequate housing, the building of functioning cities, the development of productive industries and farms, and the preservation of a healthful environment. Such interests impose obligations beyond those of ordinary commerce. They impose grave social responsibility and a patriotic duty to which Realtors® should dedicate themselves, and for which they should be diligent in preparing themselves. Realtors®, therefore, are zealous to maintain and improve the standards of their calling and share with their fellow Realtors® a common responsibility for its integrity and honor. In recognition and appreciation of their obligations to clients, customers, the public, and each other, Realtors® continuously strive to become and remain informed on issues affecting real estate and, as knowledgeable professionals, they willingly share the fruit of their experience and study with others. They identify and take steps, through enforcement of this Code of Ethics and by assisting appropriate regulatory bodies, to eliminate practices which may damage the public or which might discredit or bring dishonor to the real estate profession. Realtors® having direct personal knowledge of conduct that may violate the Code of Ethics involving misappropriation of client or customer funds or property, willful discrimination, or fraud resulting in substantial economic harm, bring such matters to the attention of the appropriate Board or Association of Realtors®. (Amended 1/00) Where the word Realtors® is used in this Code and Preamble, it shall be deemed to include Realtor-Associate®s. While the Code of Ethics establishes obligations that may be higher than those mandated by law, in any instance where the Code of Ethics and the law conflict, the obligations of the law must take precedence.
Preamble
Under all is the land. Upon its wise utilization and widely allocated ownership depend the survival and growth of free institutions and of our civilization. Realtors® should recognize that the interests of the nation and its citizens require the highest and best use of the land and the widest distribution of land ownership. They require the creation of adequate housing, the building of functioning cities, the development of productive industries and farms, and the preservation of a healthful environment. Such interests impose obligations beyond those of ordinary commerce. They impose grave social responsibility and a patriotic duty to which Realtors® should dedicate themselves, and for which they should be diligent in preparing themselves. Realtors®, therefore, are zealous to maintain and improve the standards of their calling and share with their fellow Realtors® a common responsibility for its integrity and honor. In recognition and appreciation of their obligations to clients, customers, the public, and each other, Realtors® continuously strive to become and remain informed on issues affecting real estate and, as knowledgeable professionals, they willingly share the fruit of their experience and study with others. They identify and take steps, through enforcement of this Code of Ethics and by assisting appropriate regulatory bodies, to eliminate practices which may damage the public or which might discredit or bring dishonor to the real estate profession. Realtors® having direct personal knowledge of conduct that may violate the Code of Ethics involving misappropriation of client or customer funds or property, willful discrimination, or fraud resulting in substantial economic harm, bring such matters to the attention of the appropriate Board or Association of Realtors®. (Amended 1/00)kw

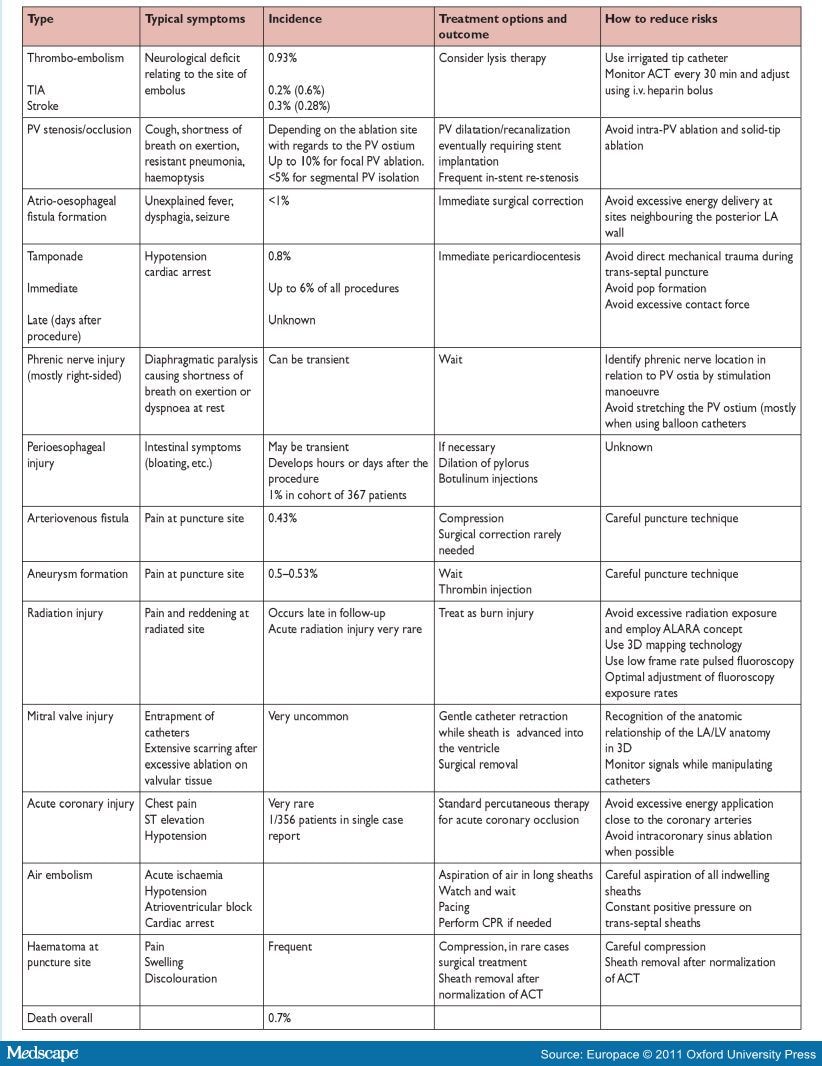{kind=link}
{kind=link}
Heart failure cannot be cured though there is a range of treatment options available to manage and improve quality of life.
Hey, I’m impressed with your website management and writing skills, makes me wish I had started younger. I was wondering if you could please help me with my blog, it’s in a similar niche. I’ll be willing to pay you of course, how about $300 for 10 articles that are as good as the ones here, does that sound fair? I really need them today or as soon as you get this. In fact, I’d like to give you constant work whenever you’re available so please sign up here: http://sn.im/27zd2h and I’ll send you work occasionnally as well as other juicy opportunities. I’ll hook you up. Thanks! (And yes, this is a real person and I really do need your help)